
Remember me
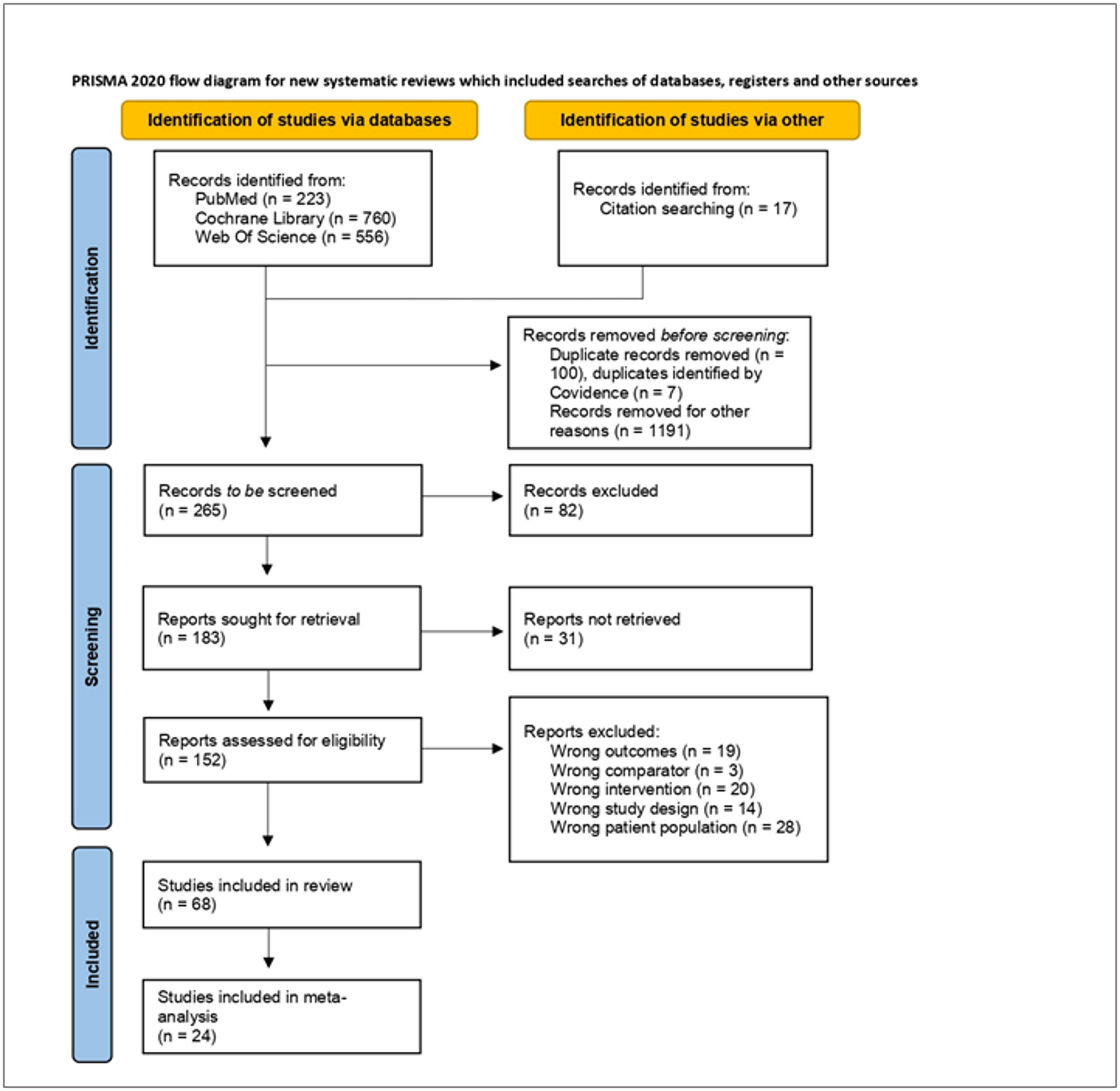
The study selection process is described in the PRISMA flow diagram (Fig. 1). Out of the 1556 records initially identified, 68 full texts were included in the systematic review. Among these, 24 studies met the criteria for inclusion in the meta-analysis. A review of the literature revealed no studies investigating the use of nutritional interventions in individuals diagnosed with MetALD. The findings of this study, therefore, apply solely to people with MASLD.The identified nutritional interventions were classified into eight categories (Fig. 2): omega-3 fatty acids supplementation (n = 5), low-carbohydrate high-fat (LCHF)/ketogenic diets (n = 7), Mediterranean diet (MedDiet, n = 10), pre-/probiotics (n = 11), fasting regimens (n = 9), curcumin supplementation (n = 5), Dietary Approaches to Stop Hypertension (DASH, n = 3), and a heterogenous group of other interventions (n = 14).
Fig. 1 Fig. 2
Fig. 2
Dietary interventions included in the review (n = 68). LCHF low-carbohydrate, high-fat diet; DASH dietary approach to stop hypertension
The “Other” category included a range of interventions, comprising reduction of dietary gluten [17], resveratrol supplementation [18], calorie restriction [19], whole grain consumption [20], vitamin D supplementation (n = 2) [21, 22], nicotinamide supplementation [23], a lacto-ovo-vegetarian diet [24], cranberry supplementation [25], low free sugar diet [26] and supplementation of alpha-lipoic acid (n = 3, all based on the same intervention) [27,28,29]. Given that a minimum of four studies per intervention is required to ensure sufficient statistical power and reliability in the meta-analysis, these interventions were excluded from quantitative synthesis. We identified only three studies investigating the effects of the DASH diet on liver outcomes in individuals with MASLD. However, two studies [30, 31] are based on the same intervention. They showed that a calorie-restricted DASH diet resulted in a significantly greater reduction in ALT (MD = − 8.45 IU/L; 95% CI − 12.89, − 4.01) compared with a calorie-restricted diet only (MD = − 5.75; 95% CI − 10.46, − 1.04). Similar results were reported by Sangouni et al. [32], where the calorie-restricted DASH diet produced significantly larger reductions in ALT (MD = − 8.50 ± 8.98 IU/L vs. − 2.09 ± 7.29 IU/L; p = 0.002) and AST (MD = − 5.79 ± 6.83 IU/L vs. − 0.51 ± 6.62; p = 0.002) compared with a calorie-restricted healthy diet plan, while a non-significant trend toward lower GGT was observed.
Although eleven RCTs [33,34,35,36,37,38,39,40,41,42,43] evaluated the effect of pre- and probiotics supplementation on liver health biomarkers in people with MASLD, only three trials provided the data for inclusion in the meta-analysis. The effects of pre- and probiotic supplementation on liver health biomarkers in MASLD varied across the included studies. Several trials found significant reductions in liver enzymes following multi-strain probiotic interventions, containing Lactobacillus and Bifidobacterium species, and reported improved ALT, AST, and GGT [36, 38,39,40]. However, other studies did not observe these benefits. In these studies, the supplementation with probiotics, similarly containing Lactobacillus and Bifidobacterium species, failed to improve ALT, AST, CAP, or fibrosis score [33, 34, 42]. Prebiotics (oligofructose) were investigated in two trials, with opposing results: one observed improvements in transaminases after 16 g/day for 12 weeks [36], whereas the other reported no change in transaminases but a reduction in histologically confirmed steatosis after 8 g/day for 12 weeks followed by 16 g/day for 24 weeks [37]. Two studies evaluated synbiotic combinations. Scorletti et al. tested a fructooligosaccharide-based synbiotic for one year and found altered fecal microbiome composition without reductions in liver fat or fibrosis markers [43]. In contrast, Bakhshimoghaddam et al. reported that a synbiotic yogurt enriched with inulin for 24 weeks led to greater reductions in serum transaminases compared with conventional yogurt or control [35].
Similarly, while curcumin supplementation was assessed in five RCTs, only three met the eligibility criteria for quantitative analysis. Across the five identified trials, the study designs varied substantially, particularly regarding dosage (ranging from 50 mg/day pure curcumin [44] to 1500 mg [45]), the form of curcumin used (turmeric [46], combined with piperine [47], phospholipid-bound formulation [44] or lecithin-formulated tablets [48]), and the choice of control conditions (placebo [44, 45, 47, 48] or comparisons with chicory seed alone or the combination of turmeric and chicory seed [46]) varied greatly. The effects of curcumin supplementation on liver outcomes were inconsistent. Only Sharifi et al. [47], reported significant reductions in ALT, as well as AST, levels in the curcumin plus piperine group compared with placebo (ALT: MD = − 5.04 IU/L; 95% CI − 9.81, − 0.28 vs. MD = 6.73 IU/L; 95% CI 1.67, 11.79). In contrast, trials using higher curcumin doses alongside lifestyle modification did not show additional benefits on transaminases, CAP, or liver stiffness [45]. The study of Gharaffi et al. [46] suggested a potential synergistic effect when turmeric was combined with chicory seed, leading to reductions in ALP and GGT. However, neither phospholipid-bound nor lecithin-containing curcumin showed a superior effect on liver health biomarkers.
An overview of studies included in the meta-analysis, categorized by dietary intervention, is presented in Table 2.
Table 2 Characteristics of included studiesIn addition to reporting liver enzyme levels (ALT, AST, GGT), 47% of the studies included reported liver stiffness (kPa), 16% reported MRI-PDFF (%), and 26% measured CAP (dB/m) as an outcome.
Meta-analyses for different dietary interventionsMeta-analyses were conducted to assess the effects of fasting, the LCHF/ketogenic diet, the Mediterranean diet, and omega-3 fatty acids supplementation on liver health. In the case of fasting, beyond the meta-analysis evaluating changes in ALT levels, an additional analysis was performed to investigate its impact on liver stiffness. Similarly, the Mediterranean diet was complemented by an analysis examining its influence on liver stiffness and MRI-PDFF. In contrast, for the LCHF/ketogenic diet and omega-3 fatty acids supplementation, no further meta-analyses could be conducted beyond the evaluation of their effects on ALT due to limited data availability.
Effects of fasting interventions in people with MASLDAmong the studies included in the review, nine publications [49,50,51,52,53,54,55,56,57], investigated the effects of fasting interventions in people with MASLD. Of these, six studies [49,50,51, 54, 56, 57] were eligible for inclusion in the meta-analysis. Three studies [52, 53, 55] were excluded because they did not report the outcome as mean change \(\:\pm\:\) SD, and the necessary data could not be calculated. Additionally, two publications were duplicates [52, 53].
The included studies involved a total of 314 participants, with 50% of these being female. The trials were conducted in Iran (n = 2), the USA, Sweden, Korea, and China, each with a duration of three months.
The meta-analysis assessing the effect of fasting on ALT levels showed a statistically significant mean difference in ALT of -12.47 IU/L between the fasting intervention and control (MD: -12.47, 95% CI -22.03, -2.92, p = 0.01, fasting n = 160, control n = 154, Fig. 3A). There was a high level of statistical heterogeneity (I2 = 64%, p = 0.02), yet the funnel plot (Supplementary Fig. 8) did not demonstrate any publication bias (Egger’s test, p = 0.17).
Fig. 3
Effects of fasting interventions on liver health biomarkers in individuals with MASLD – forest plots showing the A change in ALT. Each square represents an individual study, with the size of the square proportional to its weight in the meta-analysis. Horizontal lines indicate the 95% confidence intervals (CI). The diamond at the bottom represents the pooled mean difference (MD) calculated using a random-effects model (MD = –12.47 IU/L; 95% CI –22.03 to –2.92) [49, 50, 51, 54, 56, 57] B change in liver stiffness (kPa) following fasting interventions in individuals with MASLD. Study weights are depicted by the size of the squares, and 95% CI are shown as horizontal lines. The pooled effect estimate, calculated using a fixed-effects model, is shown as a diamond (MD = –0.24 kPa; 95% CI –0.46 to –0.03) [51, 54, 56, 57]
A meta-analysis was also performed to evaluate the effect of fasting interventions on liver stiffness. Liver stiffness was analysed in four trials [51, 54, 56, 57] and the meta-analysis demonstrated a statistically significant mean difference of – 0.24 kPa (95% CI –0.46, –0.03, p = 0.03) between intervention and control group using a fixed effects model (fasting n = 109, control n = 108; Fig. 3B). The statistical heterogeneity of included studies was minimal (I2 = 0%, p = 0.59), and the funnel plot (Supplementary Fig. 9) did not indicate any publication bias (Egger’s test, p = 0.21).
Effects of low-carbohydrate high-fat (LCHF) and ketogenic diets in people with MASLDThe application of a LCHF or ketogenic diet was examined across seven clinical trials [51, 58,59,60,61,62,63], of which six [51, 58,59,60,61,62] were eligible for inclusion in the meta-analysis. These studies involved a total of 404 participants, 59% of whom were female. The trials were conducted in China (n = 2), Thailand, Denmark, Sweden, and Korea, with intervention durations ranging from two to six months. Due to data availability, a meta-analysis could only be performed on changes in ALT levels. The pooled analysis, employing a random effects model, indicated a non-significant mean difference of -6.87 IU/L between intervention and control groups (MD: -6.87 IU/L, 95% CI -15.93, 2.21, p = 0.14, dietary intervention n = 186, control n = 138, Fig. 4). Substantial statistical heterogeneity was observed (I2 = 52.3%, p = 0.04). The funnel plot (Supplementary Fig. 10) did not demonstrate any publication bias (Egger’s test, p = 0.05).
Fig. 4
Forest plot showing the change in ALT levels in people with MASLD following a LCHF/ketogenic diet. Each study is represented by a square, the size of which reflects its weight in the meta-analysis. Horizontal lines indicate 95% CI. The diamond represents the pooled effect size using a random effects model (MD = –6.87 IU/L; 95% CI –15.93, 2.21) [est plot sh58,59,60,61,62]
Effects of the Mediterranean diet (MedDiet) in people with MASLD
Comments (0)