
Remember me
Procedures for this pilot intervention study were followed in accordance with the ethical standards of the Helsinki Declaration, current Good Clinical Practice (ICH-GCP), and the local regulatory requirements. The study protocol was reviewed and approved by the ethics committee of the School of Medicine and Health Technical University of Munich, Germany (5798/13 S-SR). Before enrolment, each participant received written and oral explanations of the study procedures, potential risks, withdrawal rights and data confidentiality. Written informed consent was obtained by trained study stuff. The study was prospectivelyregistered in the German Clinical Trials Register (DRKS: DRKS00005083), including eligibility criteria, intervention details, and prespecified outcomes.
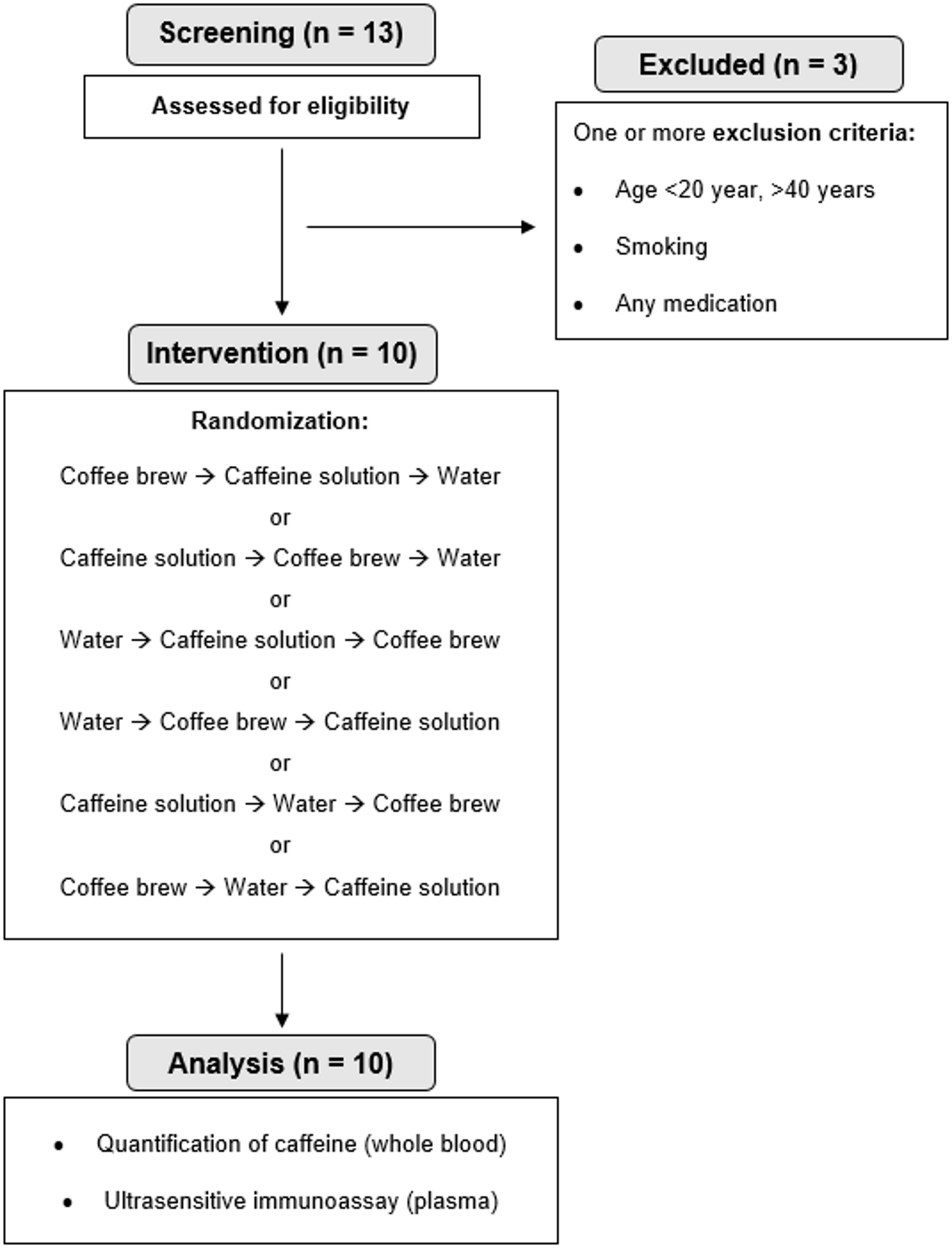
Study participants. Thirteen healthy volunteers were recruited via flyers at the Technical University of Munich, campus Freising. Enrolment of participants started on 5 November 2021, and continued until 17 February 2022. Participants’ eligibility was assessed with a detailed screening questionnaire. Exclusion criteria were age < 20 years and > 40 years, BMI > 25 kg/m2, smoking, taking any medication, practicing competitive sports and known metabolic disorders such as malabsorption syndromes, lipid metabolism disorders, diabetes mellitus, and thyroid dysfunction. To minimize interindividual variability in caffeine metabolism, tolerance, and sensory perception, only healthy individuals who regularly consumed coffee were included. This deliberate design choice enhanced the study´s internal validity and enabled more controlled interpretation of physiological responses to the intervention. Finally, ten participants were enrolled; Fig. 1 shows the participant flow chart of the study. Participants received financial compensation for their time, effort and travel expenses.
Fig. 1
CONSORT participant flow chart
Study design. Ten healthy volunteers (5 females and 5 males) participated in the pilot study. Figure 2 depicts the study design of the intervention. Each participant underwent three test days, during which they consumed one of the following: coffee brew, an aqueous caffeine solution or a water control. Blinding of participants was not feasible in this study due to the distinct sensory differences (taste, appearance and smell) between the three interventions. To minimise potential bias, a randomised crossover design was employed. Each participant received all three interventions in a randomised order. Specifically, six intake sequences were generated: (1) Coffee/Caffeine/Control, (2) Coffee/Control/Caffeine, (3) Caffeine/Coffee/Control, (4) Caffeine/Control/Coffee, (5) Control/Coffee/Caffeine and (6) Control/Caffeine/Coffee. These sequences (1–6) were randomly assigned to participant IDs using the INDEX() and RANDBETWEEN(1,6) functions in Microsoft Excel. The participants completed a one-week washout phase before the three test days, during which caffeine-containing products were not permitted to reduce potential carryover effects from habitual caffeine intake. We provided an exclusion list detailing prohibited items, including coffee products, chocolate, black/green/white tea, mate tea, cola, energy drinks, and beauty products containing caffeine (e.g., shampoos and creams). Furthermore, the study participants received a standardised meal the evening before the intervention days. As this was an exploratory pilot study, no formal power calculation was conducted. Instead, the sample size was determined based on current recommendations for pilot studies in human nutrition research [29, 30]. Specifically, we followed the guidelines outlined by Ulaszewska et al. [30], which suggest that a sample size of approximately 10–12 participants is appropriate for pilot interventions aimed at assessing feasibility and logistics, and generating preliminary data. To further illustrate the adequacy of this approach, we additionally performed a post hoc power analysis (G*Power 3.1.9.7). Assuming a medium effect size (Cohen’s d = 0.53), α = 0.05, and a power of 0.8, the required sample size was estimated as 9 participants, which was met by our final sample of 10. However, we note, that such analyses are limited, and emphasise that the primary aim of our study was not to draw definitive conclusions, but rather to inform the design of future randomized controlled trials with adequate statistical power.
Test day. On the test days, participants were in a fasted state and received either a caffeine solution (130 mg caffeine dissolved in 100 ml water, standardised to the capsules), a 100 ml coffee brew made from two capsules (one capsule contained 65 mg caffeine; Nespresso® ROMA, Nespresso Deutschland GmbH, Düsseldorf, Germany) or 100 ml water as a control. Adverse events were assessed based on participant self-report. At the end of each test day, participants were asked about whether they had experienced any discomfort, symptoms, or unusual reactions. All responses were documented.
Blood and urine samples. At the start of each test day, an intravenous catheter was inserted into an antecubital vein and remained in place until the final blood sample was collected. Blood samples were taken before coffee/caffeine/water intake (baseline = 0 h) and at defined time points (0.5, 1.0, 1.5, 2.0, 4.0, and 10.0 h) after the intervention. Six hours after consuming the beverage intake, the participants received the same standardised meal that they had eaten the previous evening. Urine samples were collected in the morning and at 1, 4, and 10 h. All samples were immediately aliquoted and stored at -80 °C until further analysis.
Standardised meals. The meal consisted of pasta (Barilla Spaghetti Nr. 5), butter, and salt (non-iodised). The pasta was cooked for 9 min and then mixed with butter and salt while still hot. The energy content of each meal was calculated based on the individual participant’s energy requirements (resting metabolic rate [RMR] x physical activity level [PAL]). One standardised meal corresponded to 1/3 of the daily energy requirement. The meal composition was based on 60% carbohydrates, 12% protein, and 28% fat. This equated to 76% pasta and 24% butter.
Calculation of individual energy demand. RMR was calculated based on gas exchange measurements performed by indirect calorimetry with the MetaLyser 3B-R3 from Cortex using a breathing mask (CORTEX Biophysik GmbH, Leipzig). Data were acquiredfor 30 min under thermoneutral conditions. To determine the individual energy demand, the RMR was multiplied with the participants individual PAL (1.2 for exclusively sedentary or reclining lifestyle, 1.4 for exclusively sedentary work with little or no strenuous leisure activity, 1.6 for sedentary work, occasionally with additional energy expenditure for walking or standing tasks, 1.8 for predominantly walking and standing work, 2.0 for physically demanding professional work) [31].
Fig. 2
Study design of the pilot intervention: all participants (n = 10) underwent the coffee brew, caffeine solution and water intervention randomly. One week before the test day, it was prohibited to consume any caffeine-containing food. The evening before the test day, participants received our standardised meal. The same meal was provided for lunch on the test day, six hours after the intervention. Blood and urine were sampled at the time points indicated. The red-circled blood samples were analysed with immune assays. Created in BioRender. Haas, M. (2025) BioRender.com/u06y391
Quantification of caffeine in human whole bloodChemicals. Caffeine (99%) and 13C3-caffeine (solution, 1 mg/ml in methanol) were purchased from Merck KGaA (Taufkirchen, Germany). Porcine EDTA blood was obtained from previous studies [32].
Standards. A stock solution of caffeine was prepared in 20% aqueous ethanol at a final concentration of 500 µM. This solution was serially diluted in 1 + 1 steps with 20% aqueous ethanol to obtain concentrations of 250, 125, 62.5, 31.3, 15.6, and 7.8 µM. An aliquot (100 µl) of each dilution was added to matrix blood (porcine blood, 900 µl) to yield matrix standards with caffeine concentrations ranging from 0.78–50.0 µM. The methanolic 13C3-caffeine-solution (1 mg/ml, Merck KGaA, Taufkirchen, Germany) was diluted to a final concentration of 10 µM with 20% aqueous ethanol and served as the internal standard solution. The matrix samples were used to prepare a calibration curve for quantitation. Additional samples (25.0 and 1.56 µM) were prepared in triplicates (n = 3) and served as quality controls (QC).
Sample preparation. The matrix standard, QC samples and authentic blood samples from the human intervention study were prepared in a similar way. An aliquot (50 µl) was subsequently mixed with the internal standard solution (50 µl) and a mixture of acetonitrile/methanol (9/1, 300 µl). The resulting suspension was then centrifuged (4 °C, 12,500 rpm, 15 min) and an aliquot of the clear supernatant was subsequently evaporated. The residue was dissolved in water (200 µl).
Calibration and quality controls (QC). Calibration standards were analysed in triplicate. The calibration curves (y = mx+b, linear regression, 1/x weighing) was [Area(caffeine/13C3-caffeine)] = 1.19 × [concentration(caffeine/13C3-caffeine)] + 0.037 (R2 = 0.998). The back-calculated standards 1.56–50.0 µM fell between 80 and 120% accuracy (81.9–111.1%) and were < 13% relative standard deviation (0.2–12.1%). caffeine eluted at 3.00 min (± 4%).
Accuracy values for back-calculated calibration standards and QC samples are summarized in Supporting Table S1 and S2.
Instrumental analysis. The chromatographic system consisted of a Shimadzu Nexera X2 ultraperformance liquid chromatography (UPLC) system (Shimadzu, Duisburg, Germany), comprising an Autosampler (SIL 30AC, kept at 15 °C), two pumps (2 × LC-30AD), a degasser (DGU 20 A5R), a column oven (CTO 30 A, kept at 40 °C), and a communication device (CBM 20 A). The UPLC system was connected to an AB Sciex 5500 Qtrap mass spectrometer (Sciex, Darmstadt, Germany) operating in positive electrospray mode. Analyst 1.6.2 was used for instrument control and data analysis. The settings were as follows: Curtain Gas, 30; collision gas, “medium”; ion spray voltage, + 5.5 kV; source temperature, 550 °C; nebulizer gas, 60; and heater gas, 60. Resolution was set to “unit”. The dwell time for each mass transition was 50 ms with 5 ms between mass transitions. Declustering potential and entrance potential were 80 and 10. MRM-traces were as follows (CE, CXP, quantifier is marked with *): caffeine 194.9 > 138.0 (27, 18), 109.9 (31, 18), 83.0* (37, 16). 13C3 -caffeine 197.9 > 139.9 (25, 20), 111.9 (31, 18), 85.9 (39, 14) 69.9* (33, 10). The samples were separated on a Kinetex C18 column (1.7 μm, 100 × 2.1 mm, Phenomenex, Aschaffenburg, Germany) with 0.1% formic acid in water (eluent A) and 0.1% formic acid in acetonitrile (eluent B) at a flow rate of 400 µL/ min. After injection (1 µl), B was kept at 5% (1.5 min) and then increased from 5% to 70% in 1.5 min followed by 0.5 min of isocratic elution. The starting conditions were re-established within 0.2 min, and equilibration was 1.3 min prior to the next injection.
Ultrasensitive immunoassayWe used the multi-array ultrasensitive MSD S-PLEX® Proinflammatory Panel 1 (Human) assay kits (MSD, Rockville, MD, USA) to quantify a panel of nine pro- and anti-inflammatory cytokines (IFN-γ, IL-1β, IL-2, IL-4, IL-6, IL-10, IL-12p70, IL-17 A, TNF). The assay uses a sandwich immunoassay format with an electro-chemiluminescent (ECL) signal to detect plasma biomarker levels in the fg/mL range. The assay performed according to the manufacturer’s, using 25 µL of undiluted plasma or quality control (QC), and all samples were analysed in duplicated in side-by-side wells. We used the MESO QuickPlex SQ 120MM (with Methodical Mind software) to detect ELC signals. Overall, three MSD S-PLEX® plates were measured, each including an 8-point calibration curve and QC samples in duplicate. Assay precision was determined by calculating the coefficient of variation (%CV) of intra-plate control replicates, yielding an average intra-assay CV of 7.58% across all plates. Consecutive data analysis was performed using MSD’s DISCOVERY WORKBENCH Version v4.0. Plasma samples collected at baseline (0 h) and after 4 h were analysed using this assay.
Calculations and statisticsBlood caffeine concentrations were calculated using Analyst 1.6.3 (Sciex, Darmstadt, Germany). The data were then analysed and visualised using GraphPad 10.3.1.
Unless otherwise stated, data in all graphs are represented as mean ± SD unless otherwise stated. For the plasma caffeine concentration plot (Fig. 3), in both panels three missing values at 4 and 10 h were interpolated using a first-order kinetic model. This model was applied using the mean values of all available data points, with the missing values being interpolated at the corresponding time points based on their maximum concentrations.
Statistical significance was assessed using paired tests based on the normal distribution, as determined by the Shapiro-Wilk-test and QQ plots. For comparisons involving two groups, either a paired t-test or a Wilcoxon signed-rank test was applied. For comparisons involving more than two groups, one-way ANOVA with Bonferroni correction (parametric) or Friedman’s test with Dunn’s multiple comparisons (non-parametric) was used.
For postprandial cytokine release, the fold change from baseline to each measurement point was calculated and presented. An asterisk (*) indicates significance between interventions, and ahashtag (#) indicates significance between baseline and the respective 4-hour measurement.
Comments (0)