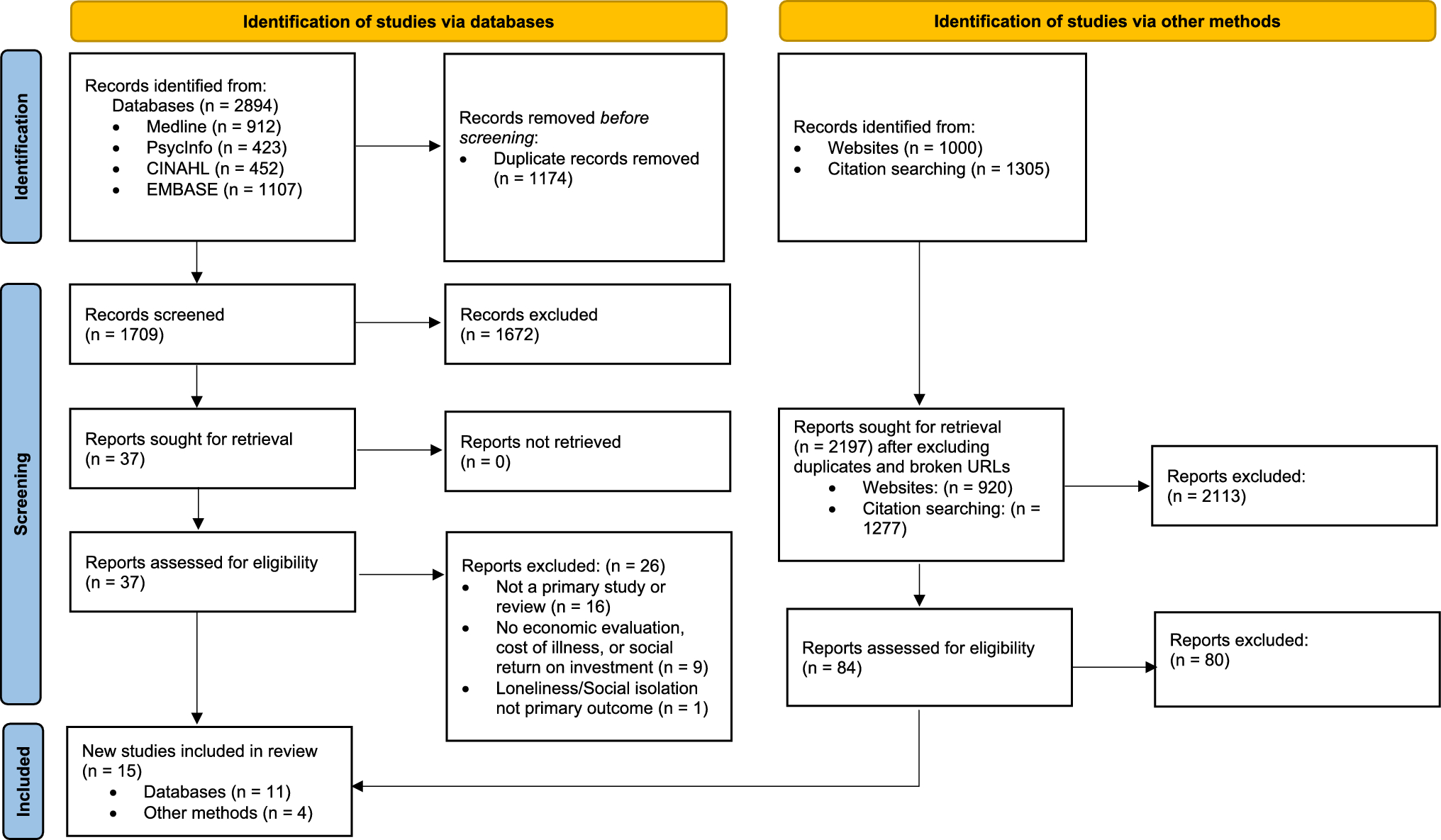
Building on a previous review that identified 12 studies [6], our updated literature review found 15 additional studies published within the last 6 years, reflecting the growing research interest in the economic impact of loneliness and social isolation. This increase in studies suggests an increasing recognition of loneliness as a public health and economic concern, prompting further investigation into its associated costs and the cost effectiveness of interventions. Despite the increase in studies, our updated review showed that most studies continue to target older adults. This was observed in the initial review, highlighting a significant knowledge gap in groups other than older adults. Studies conducted among young adults are particularly lacking, despite loneliness being as common among young adults as in older adults [30]. Another key observation is that all studies were conducted in high-income countries, predominantly in the UK. Loneliness research has largely been driven by high-income nations, and the lack of data from low- and middle-income countries has been recognised as an important equity issue [31]. There has been a notable increase in COI studies, with new cost estimates reported for countries such as Spain, Australia, the Netherlands, and Japan. This review also identified an additional COI study from the UK, which, for the first time, considered wellbeing costs and reported costs based on levels of loneliness [20]. All SROI studies included in this review assessed new interventions, but one study provided additional cost-effectiveness insights into the Friendship Enrichment Program and volunteer-led internet and computer training interventions that had been previously reviewed [22], supporting findings by Mallender et al. [32].
Our review identified six COI studies that highlighted the economic impact of loneliness and social isolation. Although all except one study [19] included healthcare costs, only three studies considered productivity costs, and only one study included presenteeism (i.e., reduced productivity at work) [20]. Two studies considered further intangible costs (expressed in loss of QALYs) [15] and wellbeing costs [20]. None of the studies focusing on older adults examined residential aged care costs, despite evidence showing that loneliness is a risk factor for care home admissions [33]. Additionally, informal care costs have not been considered by any studies, although loneliness can significantly increase informal care costs because of its association with worsened health outcomes and greater dependence on caregivers [34]. Additionally, informal carers themselves are more prone to loneliness [35]. Overall, the economic cost estimates reported in the literature are likely to be an underestimate as broader costs to individuals and our society, including foregone lifetime earnings due to worse educational and employment outcomes, have not been explored [36]. Omitting these broader economic consequences risks underestimating the true burden of loneliness and social isolation and may limit the relevance of COI findings for policy development. Where comprehensive data are lacking, COI studies should, at a minimum, acknowledge these limitations and highlight intersectoral costs as an important area for future research.
Further, most of the COI studies adopted a cross-sectional design, which limits the identification of causal relationships. Given the bi-directional relationship between loneliness and certain chronic conditions [37], longitudinal studies are needed to shed more light on whether loneliness leads to chronic conditions that lead to an increase in estimated costs or whether those who experience a chronic condition have elevated levels of loneliness, which in turn drives additional costs. Furthermore, potential mediators, such as alcohol and tobacco use, physical inactivity, and poor diet, complicate the pathways through which loneliness and social isolation contribute to chronic illness and its downstream cost consequences. These lifestyle factors are not only health outcomes in themselves but also behavioural responses that can amplify or obscure the impact of loneliness or social isolation. We identify this as a critical gap in the current literature and recommend further empirical research to quantify the role and cost implications of these behavioural mediators. In practice, we suggest future studies to present COI estimates with and without these potential behavioural mediators. Another important consideration is the necessity of controlling for confounders. Only Meisters et al. [17] controlled their cost analysis for potential confounders (demographic, socioeconomic, lifestyle-related factors, self-perceived health, and psychological distress), and their results showed that the positive association between loneliness and expenditure reversed when self-perceived health and psychological distress (using the Kessler psychological distress scale) were controlled for. Based on this finding, the authors emphasized that loneliness may influence healthcare expenditure through various pathways, including deteriorating self-perceived health and increased psychological distress.
Of the four economic evaluations, three modelled studies concluded that the interventions examined were likely cost effective. These included the Friendship Enrichment Program and volunteer-led internet and computer training [22], signposting [23], and Neighbour Day in Australia [21]. The only economic evaluation conducted alongside a trial noted that the positive psychology intervention (Happiness Route) resulted in fewer QALYs but possible cost savings [24]. However, the authors highlighted that how to interpret the results of disinvestment remained unclear given the lack of empirical studies examining the willingness-to-accept threshold for QALY losses in the Netherlands [24]. It is important to note that the two modelling studies adopted a time horizon of 5 years, which is considerably longer than the 1-year time horizon adopted in the RCT, suggesting that modelling can offer advantages in evaluating long-term outcomes and costs (although the robustness of such extrapolated impact will depend on the quality of evidence informing them). Modelling relies on effectiveness evidence, and the current evidence base for many interventions is lacking in terms of low-quality trials, small samples, lack of theoretical frameworks or understanding of loneliness, diverse undefined target groups, mixed measures of loneliness, and short follow-up periods [38]. A further observation from our review was that most economic evaluations were CUAs, using QALYs as the main measure of outcome. Although these studies used the EQ-5D and Short Form 6-Dimensions (SF-6D) measures to derive QALYs, little attention was paid to the choice of utility measure, with a previous review suggesting that utility values associated with loneliness and social isolation vary according to the choice of measure [39], which can influence cost-effectiveness results. Only one study calculated the cost per loneliness-free year gained [23], but in the absence of a cost-effectiveness threshold for improvements in such an outcome, QALYs (which are also recommended by many health technology assessment bodies) appear more suitable to facilitate comparisons. All economic evaluation studies considered healthcare costs (i.e., physician consultations, hospitalisations) in their evaluations, two modelled studies considered the costs of depression, which can be caused by loneliness [22, 23], and one study also considered costs of coronary heart disease, dementia, and stroke [23]. Productivity costs were often excluded, with the exception of Engel et al. [22], who recognised that although many older adults are no longer part of the active labour force, some continue working, and productivity costs were therefore considered. Only Weiss et al. [24] considered informal care costs, despite their importance among older adults and social care users, which can affect cost-effectiveness findings [40]. Including costs beyond the healthcare sector becomes particularly important in the context of loneliness interventions delivered outside of the healthcare system, such as school-based programmes or community engagement initiatives. To facilitate comparisons in future studies, there is an urgent need for standardised methods in economic evaluations, particularly with respect to including intersectoral costs, capturing costs associated with chronic conditions linked to loneliness, and refining measurement approaches.
Our updated review has further confirmed the growing interest in conducting SROI studies in this field, with four studies included in our review conducted in the UK. SROI studies are sometimes preferred over traditional health economic evaluations in this context because they provide a broader, more holistic assessment of the value a programme or intervention is generating [41]. This is because they allow the consideration of outcomes that go beyond health (e.g., social, economic, and environmental outcomes) and that affect multiple stakeholders (e.g., patients, carers, communities). SROI studies further place a monetary value on benefits that are considered difficult to value monetarily, such as social cohesion. Furthermore, SROI typically does not require a control group because it relies on stakeholder-informed impact measurement and valuation techniques rather than experimental designs. Instead, SROI uses counterfactual estimation, deadweight adjustment, and attribution analysis to adjust the impact [42]. Given these perceived benefits, two SROI studies in this review explicitly justified their decision to use an SROI framework instead of a traditional economic evaluation [27, 28]. However, because of the weak attribution, where a direct cause-and-effect relationship between an intervention and its outcomes cannot be established in SROI studies, and the inability to make comparisons across different health interventions due to different valuation studies, SROI studies cannot be used for economic evaluation. Additionally, it is important to note that SROI studies make it difficult to isolate the economic return specifically attributable to improvements in loneliness or social isolation, as the SROI ratio reflects the combined social value of all reported outcomes. This limitation should be taken into account when interpreting the findings.
Determining an appropriate evaluation framework for interventions targeting loneliness or social isolation requires more nuanced consideration. Interventions addressing loneliness or social isolation can be categorised into three categories: (1) individual- and relationship-level interventions (e.g., one-to-one or group interventions, digital and face-to-face interventions) focusing on maintaining and supporting people’s relationships and changing how people think and feel about them; (2) community-level strategies addressing infrastructures such as transportation, digital inclusion, and the built environment; and (3) societal-level strategies that include laws and policies, such as increasing social cohesion and reducing marginalization [43]. Although traditional economic evaluation frameworks (i.e., CEA, CUA, CBA) appear suitable for the evaluation of individual- and relationship-level interventions, it is likely that different evaluation frameworks may be required for community-level and societal-level strategies. Such interventions in a way can be considered complex interventions that contain multiple interacting components either within the intervention itself, in the delivery context, or in the way outcomes are produced. Different evaluation frameworks have been proposed for complex interventions, with some recommending the use of multiple criteria decision analysis [44] or discrete choice experiments to identify a set of attributes for complex interventions and to establish values for those attributes [45], whereas others suggested CBA or cost-consequence analysis, which seek to capture the full range of health and non-health costs and benefits across different sectors [46]. Although diversity and complexity of loneliness and social isolation interventions are acknowledged, the absence of a consistent evaluation framework poses challenges for equitable and evidence-based decision-making. The evaluation of complex interventions may necessitate moving beyond individual-reported data toward system-level data collection and the incorporation of modelling approaches. Future research is needed to establish a standardised yet adaptable evaluation framework to guide policy and resource allocation decisions.
4.1 Limitations of the Review
This review has several limitations that should be acknowledged. First, we did not include studies that exclusively examined health service use, which may have limited our understanding of the broader economic and healthcare implications of loneliness and social isolation. Second, our inclusion criteria focused only on studies where loneliness or social isolation was the primary outcome, potentially overlooking relevant studies that assessed these factors as secondary outcomes. Additionally, the use of different quality assessment checklists across studies restricted our ability to systematically compare study quality. Another limitation is that we only included articles published in English, which may have excluded relevant non-English studies. Finally, while our review focused specifically on loneliness and social isolation, we did not include studies on related concepts such as social support and social inclusion. Future research should consider these related constructs to provide a more comprehensive understanding of their economic impacts.

Comments (0)