
Remember me
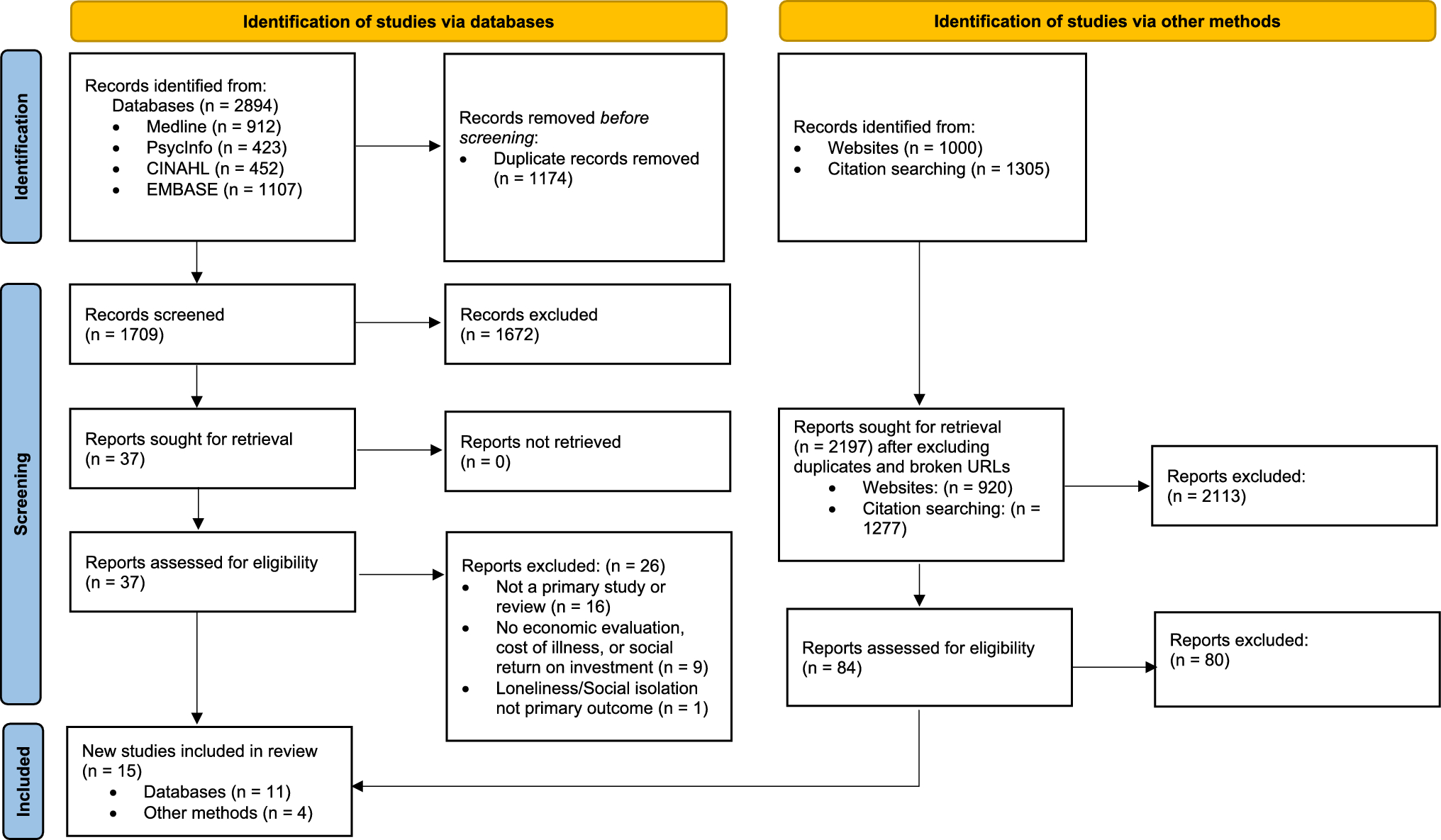
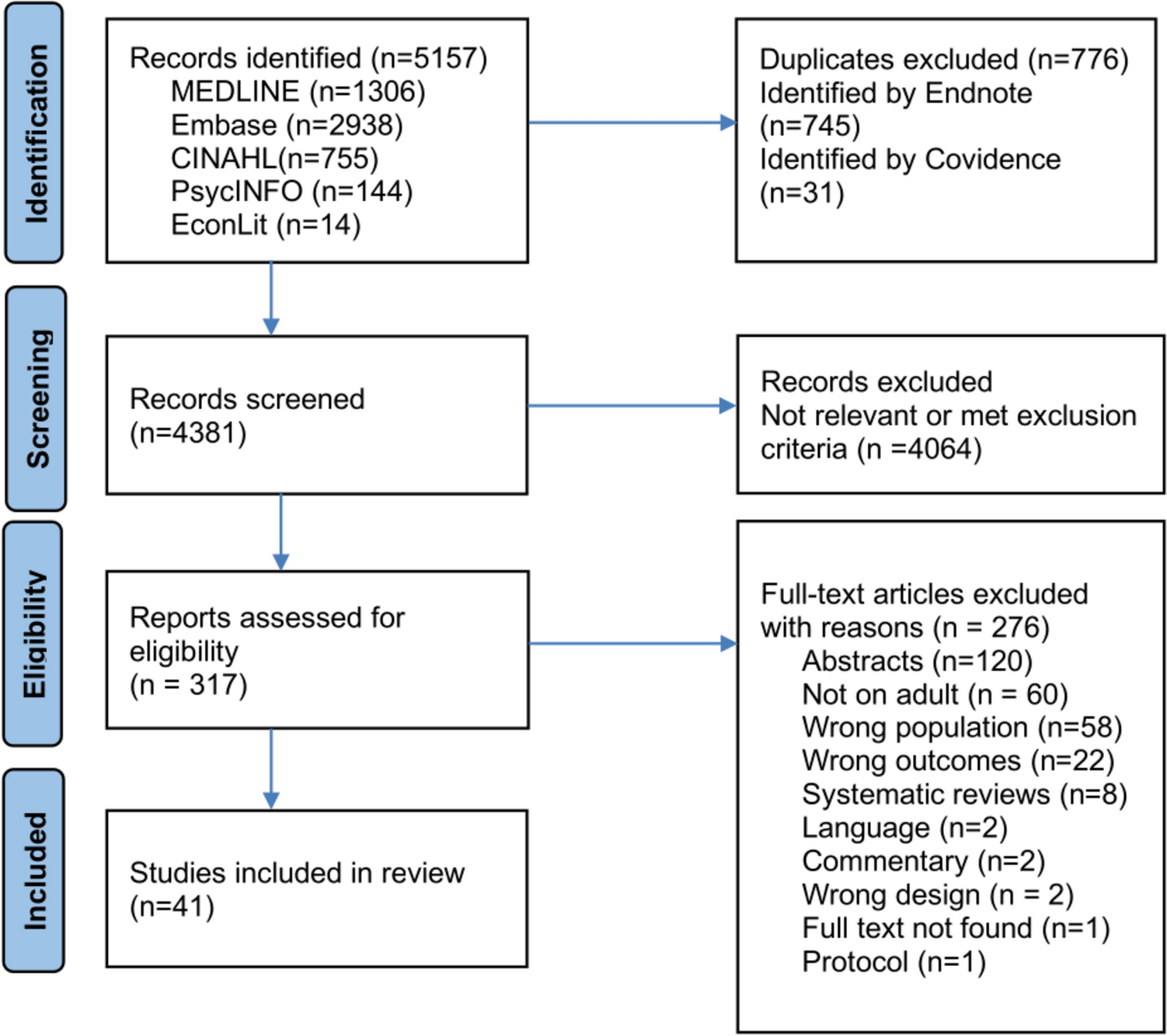
The original search of studies was conducted on 10 July, 2024, followed by an updated search on 8 April, 2025 to capture newly published studies. A total of 41 studies were included for data extraction: 25 reported on psychological burden, 15 on economic burden, and one addressed both [66]. Following the PRISMA guidelines, the detailed results are displayed in Fig. 1.
Fig. 1
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) flow diagram showing the study selection process
3.2 Characteristics of Included StudiesThe characteristics of studies are presented in Table 1. The studies were conducted across 18 countries. Most were from Asia and Europe (16 studies each), followed by North America (7 studies). The most frequently represented countries were China [59, 67,68,69,70], the Netherlands [32, 57, 71,72,73], and USA [74,75,76,77,78], each contributing five studies
Table 1 Study characteristics and key measures across included studies on the psychological and economic burden of informal caregiving for MSCs (n = 41)The studies covered a wide range of MSCs, including rheumatoid arthritis [32, 35, 57, 59, 67, 69, 72, 73, 79,80,81,82], spinal cord injuries (SCIs) [83,84,85,86], osteoarthritis [56, 76], osteoporotic fractures [66, 70, 87,88,89], fibromyalgia [76, 90], low back pain [74, 91], myotonic dystrophy type 1 [92], spinal muscular atrophy [93], and musculoskeletal injury [94]. Some studies examined the overall burden of MSC caregiving rather than specific conditions [58, 59, 68, 71].
Most psychological burden studies used cross-sectional designs, though some employed prospective cohort approaches [77, 87, 94]. Economic studies were largely based on a cost-of-illness (COI) analysis (n = 11) [70, 80, 81, 88,89,90,91, 95,96,97,98], with the majority adopting a societal perspective; one study used a payer perspective [97]. The timeframe over which informal care costs were varied across studies, with 1 year being the most common (n = 10) [73, 80, 81, 88,89,90,91, 95, 96, 98]. Sample sizes ranged widely across the studies, from as few as 43 participants in cross-sectional surveys [92] to more than 57,000 participants in registry-based economic evaluations [89], with larger studies using registries or surveys [88, 89, 91, 99].
3.3 Risk of Bias AssessmentA total of 26 psychological burden studies were evaluated using the CASP framework, with the majority (over 85%) scoring high overall quality, having met at least 75% of applicable checklist items. All studies met the criteria for addressing focused research questions and using appropriate methods. However, limitations were evident across several domains. Recruitment processes were unclear in some studies [57, 66, 86, 87]. Approximately one third of studies [32, 35, 76, 79, 85, 92, 93] lacked sufficient participants to minimize the role of chance. Furthermore, one study was rated as “No” for applicability to local populations, limiting generalizability [69] (Table 1 of the ESM).
All economic burden studies met the criteria defined in the study characteristics checklist (Table 2 of the ESM). Some studies were rated lower in quality owing to the absence of subgroup data [70, 82, 97, 99], which may be important for understanding the impact of MSC severity and type. Sensitivity analyses were not conducted in most studies [66, 70, 73, 78, 80,81,82, 88, 95, 97] and several lacked discussion of generalizability [66, 70, 72, 73, 98], or distributional implications [70, 88, 91, 96, 98, 99], limiting the applicability of findings to broader settings.
3.4 Characteristics of Caregivers from Included StudiesCaregivers were predominantly middle-aged or older, typically in their late 40s to early 60s, though some studies included younger caregivers [66, 85]. Most psychological burden studies reported female caregivers [32, 57, 59, 66, 68, 69], whereas three economic studies reported a male majority, with the percentage of male caregivers having a range from 68% [66] to 76% [72]. Some studies did not specify participants by sex. Most caregivers were primary caregivers, typically spouses or close family members [32, 35, 57]. Disease duration and caregiving time varied widely, with some studies reporting over a decade of caregiving [32, 57], while others lacked this information [
Comments (0)