
Remember me
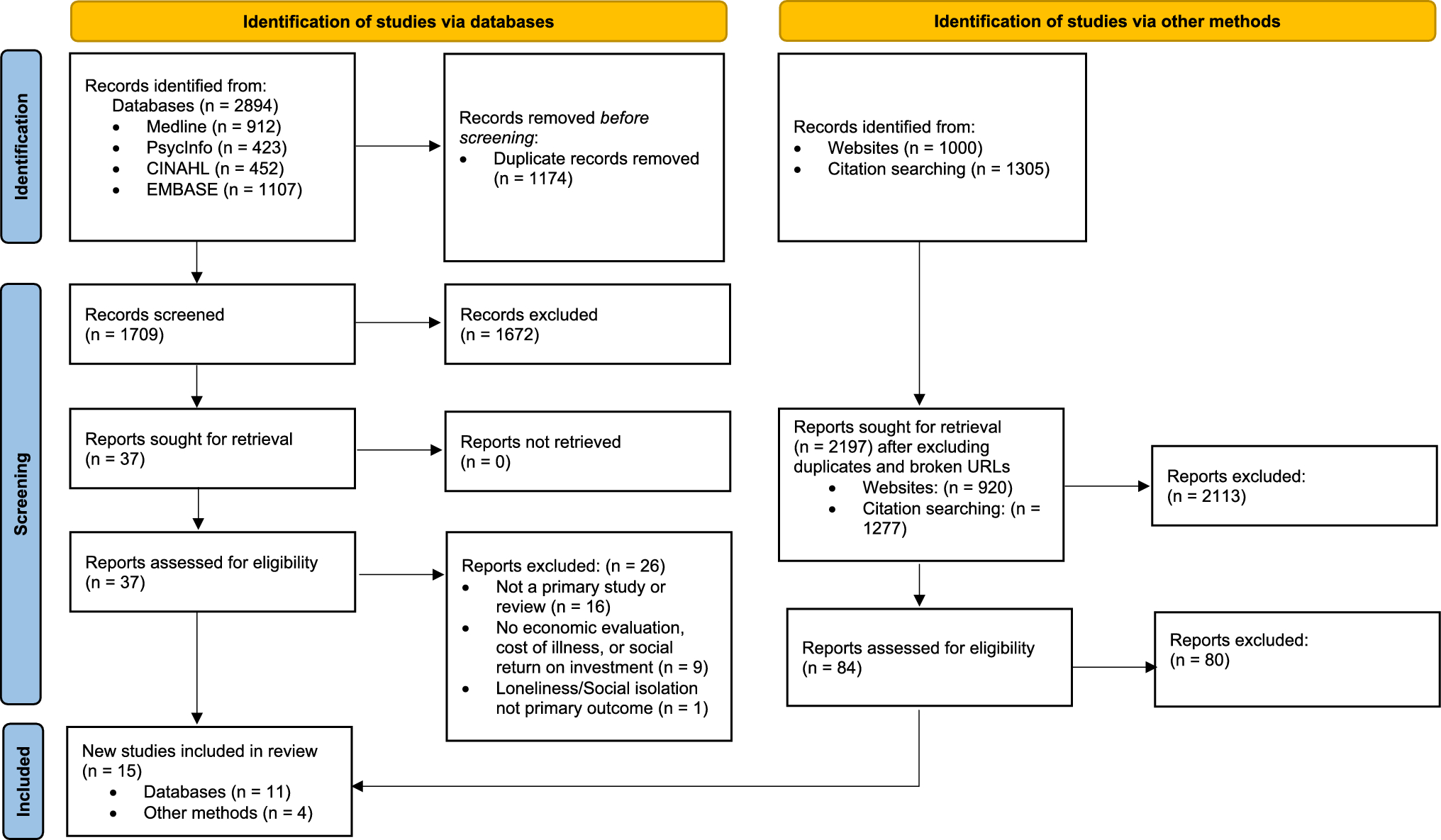
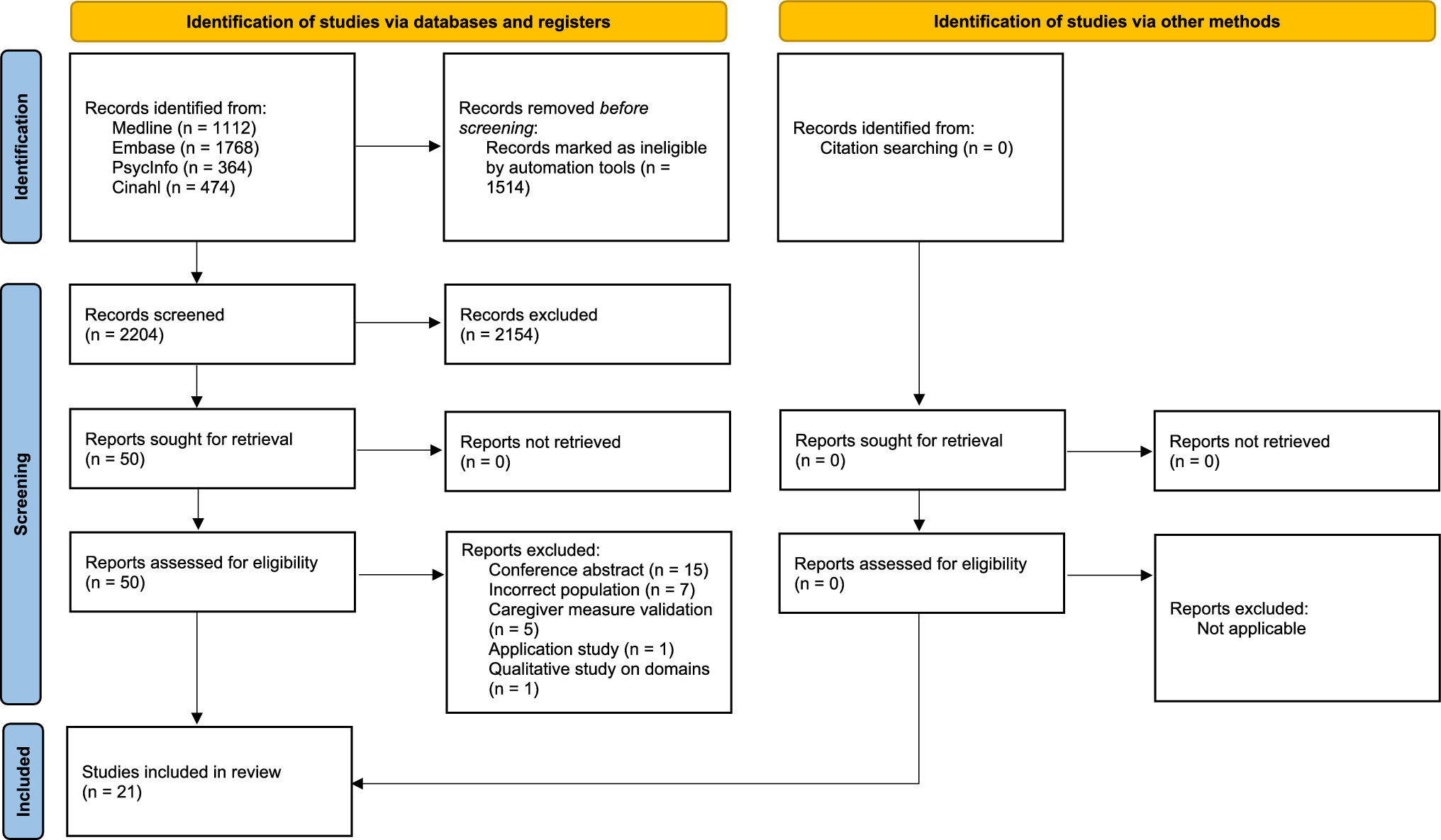
The literature search retrieved 3718 studies. After 1514 duplicates were removed, 2204 underwent the title and abstract screening process, with 2154 further studies being excluded. From the 50 studies that underwent full-text screening, 29 articles were excluded. Reasons for exclusion were conference abstracts, incorrect population (patient or proxy responses), caregiver measure (non-GPBM) validation, application and qualitative studies. There were 21 articles identified from the literature search. The Health-related Quality of Life Instrument with 8 Items (HINT-8) [34], a new GPBM that was not part of the original search strategy was identified during the screening process. A forward and backward citation search in Scopus did not find further studies. The percentages of agreement between screeners were 97% for title and abstract screening and 87% for a full-text review (Fig. 1).
Fig 1
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ; 2021;372:n71. https://doi.org/10.1136/bmj.n71
3.2 Study CharacteristicsTable 1 provides a detailed summary of characteristics of the included studies. There were 12 studies that tested a single GPBM (EQ-5D-3L, n = 5; EQ-5D-5L, n = 3; EQ-HWB-9, n = 2; HUI2, n = 1; QWB-SA, n = 1) [35,36,37,38,39,40,41,42,43,44,45,46], with the remaining studies (n = 9) testing two or more GPBMs [34, 47,48,49,50,51,52,53,54]. The EQ-5D-3L was evaluated in a total of nine studies [39, 42,43,44,45, 48, 49, 53, 54], whereas the EQ-5D-5L was tested in eight studies [34, 40, 41, 46, 47, 50, 51, 54]. One study compared the EQ-5D-3L and the EQ-5D-5L [54]. The EQ-HWB-9 [36, 37, 50, 51] and the SF-6D version 1 (SF-6Dv1) [47, 48, 52, 53] each had four studies and the HUI3 had two studies [49, 52]. The HINT-8 [34], HUI2 [38] and QWB-SA [52] had one study each. No studies were identified for 15D or the AQoL measures.
Table 1 Study characteristics by patient populationOnly limited countries were represented by the included studies. The USA was most represented by six studies [35, 38, 39, 48, 50, 52], followed by the UK [41,42,43,44, 47] and China [40, 45, 53, 54] with four studies each and three studies from Australia [36, 37, 46]. Italy [51], Iran [49] and South Korea [34] contributed one study each. The final study included informal carers from three countries, the UK, Germany and France [43].
3.3 Population CharacteristicsIn terms of the care recipients, there were six studies focusing on children care recipients with mostly parent carers [36, 37, 39, 47, 48, 52] across health conditions that included craniofacial malformations [52], meningitis [47], autism [39, 48] and non-specific conditions [36, 37]. There were eight adult care recipient studies [35, 40, 42, 45, 49, 50, 53, 54] with various carers (i.e. spouse/partners, parents, children, relatives, friends). The health conditions also varied in the adult care recipient studies, from non-specified conditions [50] to adults using long-term or social care [42] to multiple sclerosis [49] and cancers (e.g. leukaemia, colorectal and breast) [35, 40, 45, 53, 54]. For older adults, there were six studies that primarily involved spouse/partners and children as the carers [34, 38, 41, 43, 44, 46]. Five studies were in cognitive diseases, such as Alzheimer’s disease and dementia [34, 38, 43, 44, 46], with a further study in care recipients with dementia, stroke, mental illness or rheumatoid arthritis [41]. The last study compared informal carers and non-carers in the general population [51].
3.4 Psychometric Criteria OverviewTable 2 provides an overview of the psychometric criteria by the identified studies, and organised according to patient population (i.e. children, adults, older adults and general population). All GPBMs, except the HINT-8, had evidence of known-group validity from 17 studies [36,37,38,39,40,41, 43, 45,46,47,
Comments (0)