
Remember me

In 2021, the global number of BCa cases was 540,310, with a 95% UI range of 494,721 to 582,579 cases, a significant increase of 107.7% compared with that in 1990 (Table 1). The ASIR in 2021 was 6.35/100,000 (95% UI 5.80/100,000 to 6.85/100,000), showing a 7.97% decrease from 1990 (6.9/100,000, 95% UI 6.4/100,000 to 7.23/100,000). The EAPC had an overall downward trend in ASIR [EAPC = − 0.36% (95% CI − 0.41 to − 0.3)] between 1990 and 2021 (Table 1).
Table 1 Global incidence, deaths, prevalence, and DALYs of bladder cancer from 1990 to 2021From 1990 to 2021, the number of deaths due to BCa rose by 80.13% globally. In 2021, the number of deaths and ASMR were 221,888 (95% UI 200567 to 242326) cases and 2.68/100,000 (95% UI 2.42/100,000 to 2.93/100,000), respectively (Table 1). The EAPC for ASMR during the study period was − 0.98% (95% CI − 1.03 to − 0.94), showing a decreasing trend (Table 1).
Globally, the number of DALYs in 2021 was 43,970,067 (95% UI 40,636,657 to 48,136,555) cases, an increase of 60.88% from 1990. The ASDR for BCa in 2021 was 51.58/100,000 (95% UI 47.56/100,000 to 56.42/100,000), which was lower than that in 1990 (71.05/100,000 (95% UI 64.72/100,000 to 75.17/100,000). The EAPC of the ASDR of BCa [EAPC = − 1.19% (95% CI − 1.24 to − 1.13)] from 1990 to 2021 showed a decreasing trend (Table 1).
The global BCa prevalence increased 127.64% from 1990 to 3,025,553 cases (95% UI 2,823,191 to 3,224,009) in 2021 (Table 1). Its ASPR in 2021 showed an upward trend different from ASIR, ASMR, and ASDR, rising from 33.41/100,000 (95% UI 31.49/100,000 to 34.81/100,000) to 34.91/100,000 (95% UI 32.54/100,000 to 37.19/100,000). Its positive EAPC showed an upward trend [EAPC = 0.1% (95% CI 0.01 to 0.19)] (Table 1).
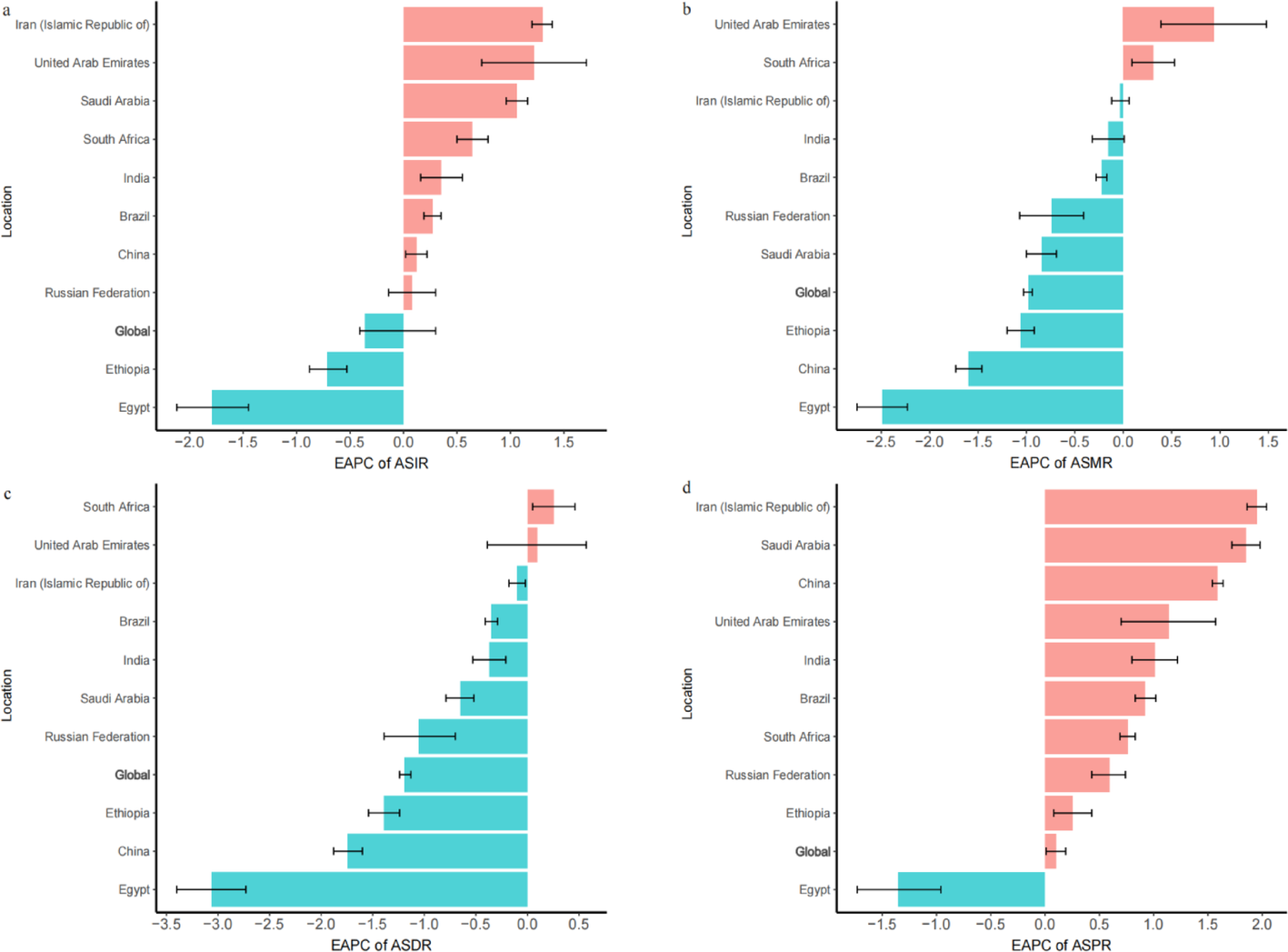
3.2 National incidence, mortality, DALYs, and prevalenceIn 2021, the top three BRICS countries with the highest ASIR were United Arab Emirates [10.28/100,000 (95% UI 7.86/100,000 to 13.15/100,000)], Egypt [9.97/100,000 (95% UI 7.01/100,000 to 17.21/100,000)], and Russian Federation [6.59/100,000 (95% UI 5.96/100,000 to 7.23/100,000)] (Table 2; Fig. 1). During the period of 1990–2021, the highest rate incidence was observed in the United Arab Emirates (717.77%), Saudi Arabia (417.89%) and Iran (334.73%). Notably, BCa also increased the most in Iran, the United Arab Emirates, and Saudi Arabia in the EAPC of ASIR (Table 2; Fig. 1a). Except for Egypt and Ethiopia, the ASIR of the remaining BRICS countries shows an increasing trend between 1990 and 2021. Egypt [EAPC = − 1.79% (95% CI − 2.12 to − 1.45)] and Ethiopia [EAPC = − 0.71% (95% CI − 0.88 to − 0.53)] had the highest decline and were above the level of decrease for global ASIR (Table 2; Fig. 1a).
Fig. 1
EAPC of the ASRs for Bladder Cancer. a EAPC of the ASIR for Bladder Cancer in BRICS. b EAPC of the ASMR for Bladder Cancer in BRICS. c EAPC of the ASDR for Bladder Cancer in BRICS. d EAPC of the ASPR for Bladder Cancer in BRICS. ASR age-standardized rate, DALYs disability-adjusted life-year, ASIR age-standardized incidence rate, ASMR age-standardized mortality rate, ASDR age-standardized DALYs rate, ASPR age-standardized Prevalence rate, EAPC estimated annual percentage change
Among the BRICS countries, China [45114 (95% UI 36263 to 57335)] and India [12904 (95% UI 11227 to 15142)] ranked the highest number of deaths due to BCa in 2021. The countries with the highest growth rate of mortality in the period of 1990–2021 were the United Arab Emirates (378.95%), Iran (218.33%), and Brazil (186.84%) (Table 2). The results of BCa ASMR after standardization were similar to the ASIR results, with the United Arab Emirates [4.6/100,000 (95% UI 3.52/100,000 to 5.82/100,000)], Egypt [4.4/100,000 (95% UI 3.13/100,000 to 7.53/100,000)], and Russian Federation [2.83/100,000 (95% UI 2.57/100,000 to 3.09/100,000)] being the three highest ranked countries (Table 2; Fig. 1b). Only the United Arab Emirates [EAPC = 0.94% (95% CI 0.39 to 1.48)] and South Africa [EAPC = 0.31% (95% CI 0.09 to 0.53)] showed an upward trend in the EAPC of ASMR in 1990–2021. Among the countries with declining burdens, Egypt [EAPC = − 2.49% (95% CI − 2.75 to − 2.23)], China [EAPC = − 1.6% (95% CI − 1.73 to − 1.46)], and Ethiopia [EAPC = − 1.06% (95% CI − 1.2 to − 0.92)] experienced a greater decline in ASMR from 1990 to 2021 BCa than the global ASMR (Table 2; Fig. 1b).
Table 2 BRICS incidence, deaths, prevalence, and DALYs of bladder cancer from 1990 to 2021Among the BRICS countries, the highest DALYs in 2021 were recorded for China [930100 (95% UI 735478 to 1185431)], India [289346 (95% UI 250585 to 342397)], and the Russian Federation [150908 (95% UI 136510 to 166266)] (Table 2). The growth rate of DALYs from 1990 to 2021 was the highest in the United Arab Emirates (435.84%), Saudi Arabia (202.53%), and Iran (176.77%). The 2021 ASDR figures for Egypt [91.71/100,000 (95% UI 65.83/100,000 to 153.7/100,000)], United Arab Emirates [87.21/100,000 (95% UI 67.29/100,000 to 110.35/100,000)], and Russian Federation [62.39 (95% UI 56.5/100,000 to 68.67/100,000)] were the highest and all were above the Global level (Table 2; Fig. 1c). Regarding the BRICS countries, the ones that showed ASDR in growth were South Africa [EAPC = 0.25% (95% CI 0.05 to 0.46)] and United Arab Emirates [EAPC = 0.09% (95% CI − 0.39 to 0.57)], while those that were below the global average were Egypt [EAPC = − 3.06% (95% CI − 3.4 to − 2.73)], China [EAPC = − 1.74% (95% CI − 1.88 to − 1.6)], and Ethiopia [EAPC = − 1.39% (95% CI − 1.54 to − 1.24)] (Table 2; Fig. 1c).
The 2021 prevalence of BCa in BRICS countries was the highest in China [570636 (95% UI 451179 to 735838)], the Russian Federation [86378 (95% UI 78111 to 94478)], and India [84172 (95% UI 72900 to 98371)]. The United Arab Emirates (898.15%), Saudi Arabia (565.59%), and Iran (402.18%) had higher growth rates of BCa prevalence in 1990–2021 than the other BRICS countries. The ASPR data for 2021 showed that the United Arab Emirates [57.03/100,000 (95% UI 44.39/100,000 to 72.67/100,000)], Egypt [54.07/100,000 (95% UI 39.06/100,000 to 89.85/100,000)], Iran [37.62/100,000 (95% UI 30.17/100,000 to 43.76/100,000 (95% UI 32.48/100,000 to 39.25/100,000)], and Russian Federation [35.93/100,000 (95% UI 32.48/100,000 to 39.25/100,000)] had higher levels of ASPR than the global average. From 1990 to 2021, among the remaining BRICS countries, the ASPR of all, with the sole exception of Egypt [EAPC = − 1.35% (95% CI − 1.73 to − 0.96)], and which evidenced a downward trend, manifested an upward progression and surpassed the global benchmark (Table 2; Fig. 1d). Iran [EAPC = 1.95% (95% CI 1.86 to 2.04)], Saudi Arabia [EAPC = 1.85% (95% CI 1.72 to 1.98)], and China [EAPC = 1.59% (95% CI 1.54 to 1.64)] had the largest increasing trend (Table 2; Fig. 1d).
3.3 Joinpoint regression analysis of BCa incidence, mortality, prevalence, and DALYs3.3.1 Joinpoint regression analysis of globalGlobally, the ASIR [AAPC = − 0.27% (95% CI − 0.32 to − 0.22), P < 0.001], ASMR [AAPC = − 0.84% (95% CI − 0.91 to − 0.77), P < 0.001] and ASDR [AAPC = − 1.02% (95% CI − 1.09 to − 0.96), P < 0.001] showed a downward trend, while ASPR [AAPC = 0.14% (95% CI 0.08 to 0.21)] showed a steady increase during this period (Table 3; Fig. 2). In terms of ASIR, only the period from 1990 to 1996 [APC = 0.71% (95% CI 0.57 to 0.85), P < 0.001] showed an upward trend. Among the other year intervals, the downward trend was most pronounced from 2010 to 2021 [APC = − 0.58% (95% CI − 0.65 to − 0.51), P < 0.001] (Table 3; Fig. 2). ASMR has shown a significant decline since 1994, with the most pronounced downward trend occurring from 2001 to 2007 [APC = − 1.50% (95% CI − 1.67 to − 1.34), P < 0.001] (Table 3; Fig. 2). Globally, the ASDR was essentially flat from 1990 to 1994, while maintaining a significant decline thereafter, with the most pronounced downward trend in 2001–2007 [APC = − 1.76% (95% CI − 1.90 to − 1.61), P < 0.001] (Table 3; Fig. 2). It is noteworthy that ASPR was in a state of growth from 1990 to 2010, with the fastest growth in 1990–1995 [APC = 1.12% (95% CI 0.90 to 1.33), P < 0.001], but in the subsequent period of 2010–2021 [APC = − 0.45% (95% CI − 0.52 to − 0.37), P < 0.001], the global ASPR of BCa begins to show a slower decline (Table 3; Fig. 2).
Table 3 AAPC of ASIR, ASDR, ASMR, and ASPR for bladder Cancer in global from 1990 to 20213.3.2 Joinpoint regression analysis of BRICS countriesIn most of the BRICS countries, the ASIR for 1990–2021 showed an overall upward trend, different from that of Global, with Russian Federation [AAPC = 0.48% (95% CI 0.00 to 0.96), P = 0.051] being the most significant, and the 1990–1994 ASIR [APC = 6.80% (95% CI 5.29 to 8.33), P < 0.001] was the time interval that influenced the increase in the overall burden of the Russian Federation of ASIR. In addition, there is also a downward trend in some of the BRICS countries, with the most significant decline in Egypt [AAPC = − 1.12% (95% CI − 1.35 to − 0.88), P < 0.001], where the 2001–2006 ASIR [APC = − 7.77% (95% CI − 8.50 to − 7.03), P < 0.001] was the most significant influence on its AAPC decline had the greatest impact (Table S2; Fig. 2).
In the study of ASMR and ASDR, it was found that the trend of AAPC in most of the BRICS countries in 1990–2021 coincided with the declining trend of Global, with Egypt [ASMR, AAPC = 1.96% (95% CI 2.31 to 1.61), P < 0.001; ASDR, AAPC = 2.46% (95% CI 2.92 to 2.00), P < 0.001] were the countries with the largest decreases in ASMR and ASDR, which declined between 2001 and 2006 for ASMR [APC = − 6.79% (95% CI − 7.84 to − 5.74), P < 0.001] and 2001–2005 for ASDR [APC = − 9.53% (95% CI − 10.60 to − 8.44), P < 0.001] period had the most rapid decline, resulting in a significant reduction in Egypt’s burden over the study period (Table S2; Fig. S1 and S2). 1990–2021 South Africa[ASMR, AAPC = 0.33% (95% CI − 0.22 to 0.88), P = 0.245; ASDR, AAPC = 0.25% (95% CI − 0.48 to 0.99), P = 0.504] was the country with the least decline in ASMR and ASDR, 1994–1997 [ASMR, APC = 6.14% (95% CI 1.26 to 11.27), P = 0.017; ASDR, APC = 5.33% (95% CI − 1.21 to 12.30), P = 1.106], with a significant increase in ASMR and ASDR values being the most significant factor influencing their results (Table S2; Fig. S1 and S2).
The ASPR of the BRICS countries grows in the same trend as Global from 1990 to 2021, with the fastest growth in Saudi Arabia [AAPC = 1.91% (95% CI 1.80 to 2.02), P < 0.001] among the BRICS countries, and the ASPR from 1990 to 1994 [APC = 4.39% (95% CI 4.07 to 4.71), P < 0.001] was the most important time period influencing the change in the overall trend of their ASPR (Table S2; Fig. S3). It is worth noting that 2001–2005 was the time period with the most significant impact on Egypt, where ASPR [APC = − 8.66% (95% CI − 9.62 to − 7.70), P < 0.001] showed a significant decline, Egypt became the only organization to show a significant decline in its overall trend of ASPR [AAPC = − 0.53% (95% CI − 0.90 to − 0.17), P = 0.004] in the period 1990–2021 in negative growth (Table S2; Fig. S3).
Fig. 2
Joinpoint Regression Analysis of the ASIR of Bladder Cancer between Global and in the BRICS Countries
3.4 Burden of BCa based on SDI3.4.1 Relationship between ASRs and SDIIn this study, the SDI values of both global and BRICS countries increased from 1990 to 2021, and the burden of ASRs for BCa in BRICS countries as a whole showed an increasing trend with the increase of SDI and reached a peak at SDI of 0.85 (Fig. 3). The higher the level of socioeconomic development, the higher the disease burden. It is noteworthy that the ASRs in Egypt were consistently higher than the expected level, while the ASRs in India, Saudi Arabia, Brazil, and South Africa were consistently lower than the expected level. In addition, United Arab Emirates’ ASRs fall back to desired levels after 2019, China’s ASIRs and ASPRs are consistently lower than desired levels, but its ASMRs and ASDRs are essentially in line with desired levels, and Ethiopia’s burden of all diseases is essentially in line with desired levels (Fig. 3).
Fig. 3
ASRs for Bladder Cancer of BRICS and Global by SDI. a–d According to SDI, ASIR, ASMR, ASDR and ASPR for BRICS countries and globally 1990–2021. SDI Socio-Demographic Index
3.4.2 Relevance of EAPC to SDIWe then delve further into the relationship between the EAPC of ASRs and the 2021 SDI. The results showed that although the correlation between ASPR (P = 0.191), ASMR (P = 0.339) and ASDR (P = 0.35) was not significant, we can find that with the increase of SDI, the EAPC showed an upward trend (Fig. 4). There was a positive correlation between EAPC of ASIR and SDI in 2021 with almost marginal correlation P = 0.064 (Fig. 4).
Fig. 4
Correlation between EAPC and SDI of Bladder Cancer and ASDR for lung cancer. a Correlation between AAPC of ASIR in 2021 and SDI in 2021. b Correlation between EAPC of ASMR in 2021 and SDI in 2021. c Correlation between EAPC of ASDR in 2021 and SDI in 2021. d Correlation between EAPC of ASMR in 2021 and SDI in 2021
3.5 Attribution risk factor analysisIn the data from the study of the incidence of risk factors for BCa development in 1990 and 2021 globally and the BRICS countries, the most important risk factor for both ASMR and ASDR of BCa was smoking, followed by HFPG, except in Ethiopia in 1990, where HFPG was the primary factor influencing their ASMR (Table S3; Fig. 5).
Comparing 1990 and 2021 data, the BCa’s disease burden of ASMR due to smoking increased globally and across BRICS countries, with the largest increase in BRICS countries being in Egypt (1.02 per 100,000) and the smallest increase in Iran (0.02 per 100,000) and Saudi Arabia (0.02 per 100,000) (Table S3; Fig. 5a). The top three BRICS countries with the highest increase in ASMR burden due to smoking in 1990 were Egypt (1.60 per 100,000), Russian Federation (0.89 per 100,000), and China (0.87 per 100,000), while in mid-2021, Egypt (2.62 per 100,000) remains unchanged, China (1.24 per 100,000) rises to second place among the BRICS countries, and United Arab Emirates (1.16 per 100,000) rises to third place (Table S3; Fig. 5a). Compared to 1990, only China (0.17 per 100,000) and Ethiopia (0.14 per 100,000) have higher ASMR burdens due to HFPG in 2021, with China having the largest increase (0.03 per 100,000) (Table S3; Fig. 5a).
Fig. 5
Trends in attributable risk factors for bladder cancer death and DALY in the world and BRICS countries in 1990 and 2019. a ASMR attribution analysis for 1990 and 2021. b ASDR attribution analysis for 1990 and 2021
It is interesting to note that the burden of ASDR due to smoking decreased to varying degrees globally and in all BRICS countries during the observation period, with the largest decrease in Egypt (29.48 per 100,000), where the burden of ASDR due to smoking was consistently the third highest in 1990 and 2021 in Egypt, the Russian Federation, and the United Arab Emirates. Emirates consistently ranked among the top three countries in terms of the burden of ASDR due to smoking (Table S3; Fig. 5b). Among the risk factors HFPG, only three countries showed a decreasing trend in the burden of ASDR due to HFPG, namely China (2.49 per 100,000), Ethiopia (1.95 per 100,000), and United Arab Emirates (10.01 per 100,000), with China showing a decreasing trend. China (0.69 per 100,000) (Table S3; Fig. 5b).
3.6 Predictions of the disease burden of bladder Cancer from 2022 to 20363.6.1 Trend predictions of incidence, mortality, DALYs and prevalence of bladder Cancer globallyThe study provides BAPC projections of BCa ASRs globally for the years 2022–2036. It was concluded that ASIR, ASMR, ASDR and ASPR of BCa globally had a high probability of showing a downward trend development during the study period. In particular, ASIR in 2036 is projected to decrease to 5.8 (per 100,000), ASMR is projected to decrease to 2.2 (per 100,000), ASDR is projected to decrease to 45 (per 100,000) and ASPR is projected to decrease to 32 (per 100,000) (Fig. 6a-d).
Fig. 6
The assessment results of the ASRs of global bladder cancer from 1990 to 2021 and the predictions of ASR values from 2022 to 2036. a The prediction results of the ASIR of bladder cancer globally. b The prediction results of the ASMR of bladder cancer globally. c The prediction results of the ASDR of bladder cancer globally. d The prediction results of the ASPR of bladder cancer globally
3.6.2 Trend predictions of the incidence, mortality, DALYs and prevalence of BCa in the BRICS countriesThe ASIR for BCa in the BRICS countries predicted using Bayesian modeling for the period 2022–2036 shows a more polarized picture, with Brazil, Iran, Russian Federation, South Africa and United Arab Emirates showing a downward trend similar to the Global trend, while China, Egypt, Ethiopia, India and Saudi Arabia on the contrary predict a more pronounced upward trend (Fig. 7). In the projections of ASMR burden for the BRICS countries, with the exception of Egypt and Ethiopia, which show an increasing trend, the rest of the BRICS countries show varying degrees of decline, and it is worth noting that Ethiopia’s ASMR burden, although it rises during the period of 2022–2036, rises slowly and reaches a maximum in 2036 that is still below the historical peak (Figs. S4 and S5). In the projections of ASDR burden, China, Egypt, Ethiopia, and South Africa show increases that contradict the global trend, but all have slower increases and peaks that are still not higher than historical peaks over the projection period. In the ASPR outcome projections, only Iran, the Russian Federation and the United Arab Emirates in the BRICS countries show the same downward trend as the Global projections, with the Russian Federation’s projected ASPR burden showing a less pronounced decline (Fig. S6).
Fig. 7
Projects the ASIR in bladder cancer for a Brazil, b China, c Egypt, d Ethiopia, e India, f Iran(Islamic Republic of), g Russian Federation, h Saudi Arabia, i South Africa and j United Arab Emirates from 2022 to 2036
Comments (0)