
Remember me

The implants developed in this work consisted of a pellet and a tubular rate controlling membrane formulated with biodegradable polymers. These membranes are prepared using a tubular shape and contained three types of PCLs as described previously [34, 35]. These membranes presented a porous structure that controls drug permeation. In the present powork these membranes were prepared by casting a polymeric solution on the surface of a rotating rod. The resulting membranes had a cylindrical shape with a thickness of approximately 183 ± 6 μm. The thickness of the membranes falls within the range (100–200 μm) reported previously for similar biodegradable rate controlling membranes prepared for implantable devices [36,37,38,39].
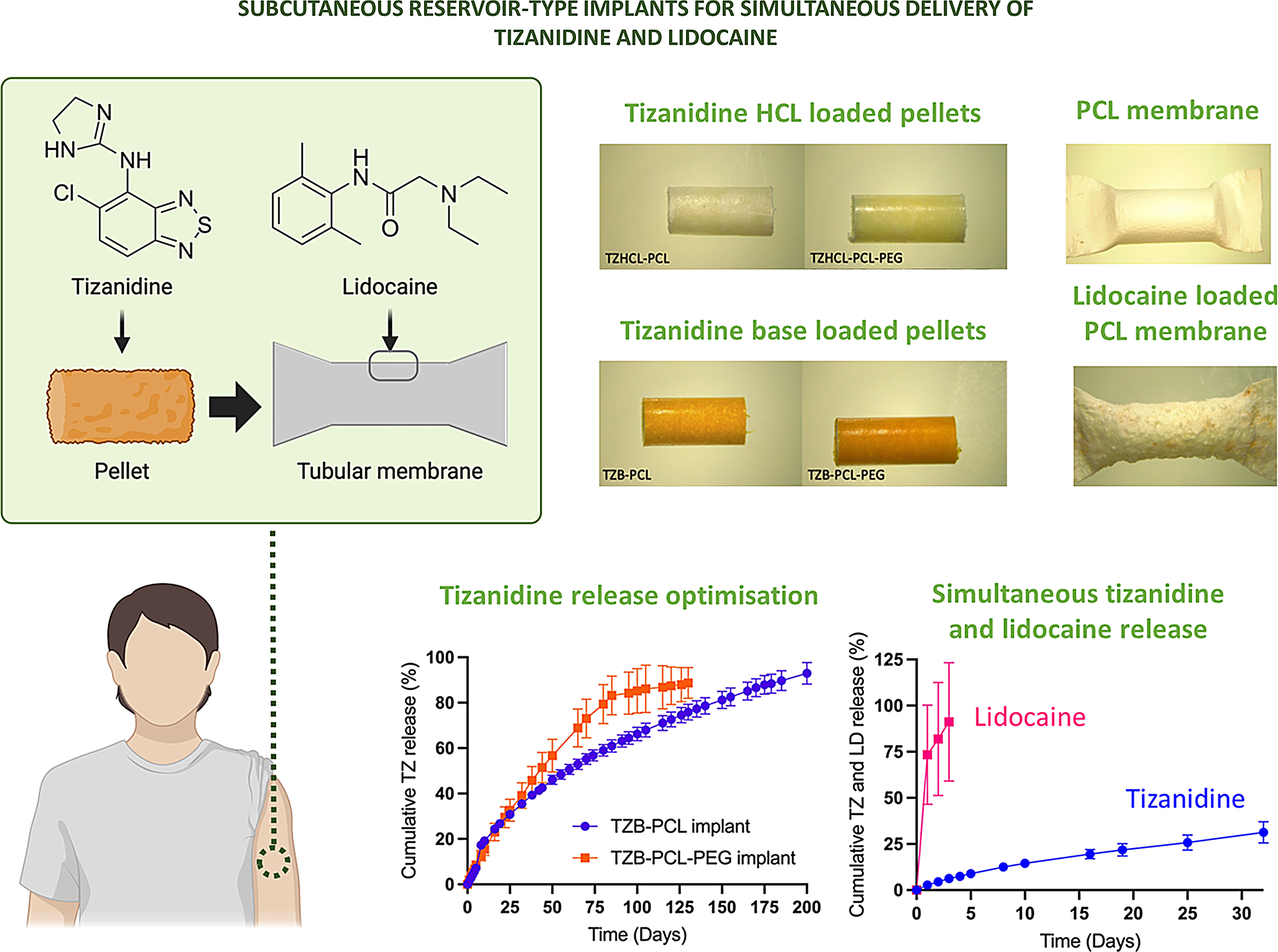
Preparation of pelletsPellets containing TZ and different excipients (PVP, HPBCD, and PCL) were developed by direct compression. The resulting mini tablets have a cylindrical shape designed to be introduced inside the tubular membrane. PCL was selected as a biocompatible, biodegradable polymer capable of controlling drug release over extended periods [40, 41]. Additionally, it is more cost-effective than alternatives such as poly(lactic-co-glycolic acid), helping to keep the overall device cost low [42]. In the case of PCL, the manufacture of the pellets was more challenging. Even though the biodegradable nature of PCL makes it an ideal polymer to prepare implantable devices, this polymer is not suitable for direct compression. Directly compressed PCL pellets did not show good cohesion. It was challenging to remove them from the die and handling them without breaking them. This can be due to PCL properties or to the material particle size that was larger than the one of PVP and HPBCD. Therefore, an alternative manufacturing method for PCL-based pellets was used. Pellets with drug and polymer (PCL or PCL-PEG) in equal mass proportions (50%) were prepared using a melt-processing technique. To ensure a homogeneous distribution of the drug in the implant, a method involving the preparation of drug-polymer films was employed. Subsequently, a portion of the resulting film was melt-processed in the VCM equipment to prepare the resulting drug loaded pellets. The resulting implants took the form of cylindrical rods with dimensions of approximately 2.9 mm in diameter and 15 mm in length (Fig. 1). This size was selected to evaluate implant prototypes. The shape and size of an implant device can significantly impact its effectiveness, safety, and patient comfort [43]. It is important for the delivery method of the device. If the overall size exceeds the capacity for insertion via tools like a trocart, surgical incision becomes necessary. Considering that these pellets are designed to be implanted subcutaneously, they present attributes like a compact size and cylindrical shape to fit in the body with a minimally invasive injection. The implants prepared present similar diameter than commercially available implants such as Nexplanon and shorter length [44]. However, larger implants can be prepared as cylindrical implants of up to 4 cm in length and up to 4 mm in diameter have been described [44]. Indeed, more than one of these pellets can be loaded inside the PCL membranes to provide higher dosages if needed. This could allow the development of implants with different dosage adapted to patient’s needs.
It is important to note that solvent use was included to ensure proper mixing of the drug and polymer. While VCM replicates the melt-processing of hot melt extrusion, it lacks equivalent mixing efficiency. Therefore, solvent casting provides a suitable alternative, as previously reported [45]. DCM has been used in pharmaceutical manufacturing, such as in tablet coatings. However, the FDA advises controlling DCM levels to minimise toxicity risks. Our analysis of similar implants confirmed that residual DCM content remained below the FDA’s recommended limit of 50 ppm [46]. Additionally, cytotoxicity assessments of implants and membranes produced with DCM demonstrated no cytotoxic effects [32, 46, 47]. This can be applied to the membranes described in the "Preparation of membrane" section.
Effect of excipient on the formulation of TZ hydrochloride and TZ baseMicroscopy examination (Microscopy, SEM, RAMAN)The morphology of all the formulations was examined under the microscope. Pellets developed by direct compression presented a rugged surface, related to the powder’s mixture, whereas pellets formulated by VCM had a smooth surface without the presence of bubbles, and the drug was well dispersed throughout the formulation (Fig. 1). The pellets containing TZ in its base form appeared orange due to the presence of the drug. To examine the morphology of the pellets in more detail, SEM was utilised (Fig. 1). The images depicted the presence of TZ and polymer in the all the pellets, with further dispersion evident within their structure, as discernible clusters of drug crystals were not apparent. Interestingly, TZB-based implants appear to have a smoother surface than TZHCl-based implants. This could be because, during the mixing process, both the polymer and the drug were dissolved in an organic solvent to cast films. TZB has higher hydrophobicity, allowing for better mixing and integration with the hydrophobic polymer matrix. Despite this, direct compression and VCM seem to be an appropriate method to prepare drug containing pellets for the development of implantable devices.
One of the most common ways to develop pellets is by extrusion-spheronization [48]. However, VCM and direct compression has been described previously as valuable ways of preparing drug loaded pellets [29, 49,50,51].
Fig. 1
Images of pellets using the Leica E24W microscope at x8 magnification of (a) TZHCL only, (b) TZHCL-PVP, (c) TZHCL-CBD, (g) TZHCL-PCL (h) TZHCL-PCL-PEG, (i) TZB-PCL, and (j) TZB-PCL-PEG. Scale bar: 2 mm. SEM images of (d) TZ only, (e) TZHCL-PVP, (f) TZHCL-CBD before release; TZHCL-PCL (k) before and (o) after release, TZHCL-PCL-PEG (l) before and (p) after release, TZB-PCL (m) before and (q) after release, and TZB-PCL-PEG (n) before and (r) after release at X500 magnification with a scale of 200 mm
Moreover, those pellets made by VCM were examinate using MicroCT (Fig. 2a), to verify the lack of holes or bubbles inside the tablets. All the formulations presented a solid core with the drug and polymers well distributed in the matrix, as it was demonstrated previously. Interestingly, the appearance of the pellet cross-sections shows similar results to those obtained in the SEM analysis. TZB-based implants appear smoother than the surface of TZHCl-based implants. This has been attributed to a better mixture between hydrophobic TZB and PCL compared to TZHCl. Additionally, this finding was supported by Raman spectroscopy analysis of the implant cross-sections (Fig. 2b–c). To assess drug distribution within each pellet, we mapped the intensity of the TZ peak at ca. 1350 cm⁻¹, as neither PCL nor PEG exhibited peaks at this specific Raman shift (Fig. 2b). The results suggest that the drug is distributed across the surface of the implant but in TZHCL-based implants there are obvious drug spots (Fig. 2c). This high drug concentration spots are consistent with the roughness previously reported for this type of implants. This phenomenon is more obvious for TZHCL-PCL than for TZHCL-PCL-PEG. The presence of PEG in the later contributes to drug solubilisation within the polymer matrix. Despite the presence of high drug concentration domains, the rest of the surface of the implant contains drug. This behaviour has been observed before for other types of implants that contain drug crystals dispersed within a polymer matrix [52, 53]. Therefore this is not considered a problem in the formulation but this phenomenon might influence drug release kinetics.
Fig. 2
µCT images showing the cross-section of a pellet prepared using VCM (a). Raman spectra of the pure compounds used in the preparation of TZ-containing pellets (b), and Raman mapping of the cross-section of pellets prepared using VCM (c). The white bar in the Raman spectroscopy images represents 200 μm. The colour scale indicates peak intensity for the drug peak at approximately 1350 cm⁻¹, with the minimum representing 0 intensity and the maximum values as follows: 8422 for TZHCl-PCL, 2626 for TZHCl-PCL-PEG, 6560 for TZB-PCL, and 5455 for TZB-PCL-PEG
Thermal analysis: differential scanning calorimetry and thermal gravimetric analysisThe thermal behaviour of the drug in its isolated form and mixing with polymer, as well as the raw powders of the polymers, were analysed using DSC. Thermograms (Fig. 3) for samples containing PCL and PCL-PEG combinations displayed a distinct endothermic peak at approximately 55 °C, corresponding to the melting points of both PCL and PEG [47, 54, 55]. Notably, when PCL and PEG were combined, the peak became slightly broader, suggesting interactions between the two polymers. These findings align with previous studies on PCL-PEG blends prepared via hot melt extrusion, where PEG was reported to act as a plasticiser for PCL [55]. On the other hand, thermograms, revealed a distinct endotherm peak at 296 °C, corresponding to the fusion of TZHCL, whereas the formulations developed exhibited a noteworthy shift in peak temperature towards lower values (295 °C for TZHCL-PCL and 291 °C for TZHCL-PCL-PEG). This observed difference in the temperatures of fusion between the pure drug and the formulation could be attributed to an interaction between TZHCL and the polymer matrix. On the other hand, the thermogram showed an endothermic peak of TZB at 225 °C, corresponding to the fusion of the drug. The behaviour of the drug base is slightly different as the change in the DSC melting peak is more dramatic. When TZB was combined with polymer (PCL, PEG) the melting peak showed a shift to lower temperatures (219 °C for TZB-PCL and 213 °C for TZB-PCL-PEG) and present a broader shape indicating a reduction in drug crystallinity. Moreover, the effect is more obvious when PEG was incorporated into the mixture. This is consistent with a more even drug distribution obtained in the Raman analysis (Fig. 2). Also, this behaviour was previously reported for PCL/PEG based implants containing olanzapine [56]. Interestingly, drug melting peaks are sharper and more intense for TZHCL-based pellets indicating a higher degree of crystallinity. These results are consistent with the findings reported previously suggesting that the hydrophilic drug salt present domains of high crystallinity within the polymer matrix.
Alternatively, TGA analysis (Fig. 3) shows that the degradation of drug loaded pellets starts at higher temperatures than pure drug confirming the results obtained in DSC. The observed thermal behaviour conforms to the typical patterns exhibited by eutectic mixtures, where interactions such as adhesion forces are prevalent within the system, as documented in previous works [57,58,59,60]. These interactions can contribute to reduce drug crystallinity as evidenced by the drug melting point shift to lower temperatures. Equivalent behaviour was reported for other drugs such as risperidone or olanzapine when combined with PCL or PCL/PEG mixtures respectively [34, 61]. Polymer/drug interactions and changes in crystallinity can be evaluated using XRD and FTIR spectroscopy.
Fig. 3
DSC traces for (a) pellets containing TZHCL and (c) pellets containing TZB. TGA curves for (b) pellets containing TZHCL and (d) pellets containing TZB
Attenuated total reflectance fourier transform-infrared spectroscopy analysis (FT-IR)To understand the physicochemical properties and functionality of all formulations, FTIR studies were conducted. Spectra of drug powder, polymers, and mixtures of these components are shown in Fig. 4. Characteristic peaks of TZHCL were observed at 672 cm− 1 related to aromatic bending, 945 cm− 1 corresponding to aromatic C-Cl stretching, 1645 cm− 1 and 1606 cm− 1 corresponding to C = C bonds, and 3246 cm− 1 related to a secondary amine group [62, 63]. These peaks were evident not only in the spectra of the drug alone but also in the spectra of the pellets, demonstrating the effective integration of the drug into the matrix of the formulated implants. Characteristic peaks of PCL, such as the peak at 1723 cm− 1 corresponding to the C = O bond, and 1240 cm− 1 correlated to C-O-C stretching [64, 65], as well as PEG indicated by the peak at 1099 cm− 1 corresponding to C–O–C stretching [66, 67], were also present in the implants.
The obtained formulations containing PCL only did not show shifts in the absorption bands characteristic of the drug and the polymers, nor did new bands emerge. However, in the TZHCL-PCL pellet, the high intensity in the absorption bands corresponding to the polymer in the mixture appeared to mask some characteristic bands of the drug. Upon detailed analysis of these respective peaks, it was observed that there were no new absorption bands or shifts in the characteristic peaks of the drug, confirming previous observations. Formulations containing a PCL-PEG combination showed a peak shift at 1604 cm⁻¹, suggesting non-covalent interactions between the drug and the polymer matrix. Additionally, a slight shift in the TZHCl amine peak at around 3200–3400 cm⁻¹ was observed in PCL-PEG implants. This shift has been associated with hydrogen bonding between the drug’s amine groups and carbonyl groups [68]. Given that this effect is more pronounced in PEG-containing pellets, we can hypothesise that the hydrogen bonds form between the amine groups of TZHCl and the oxygen groups in the PEG chains. This finding is consistent with the melting point shift presented in the DSC analysis. These results are consistent with previously reported for olanzapine implants prepared using PCL and PCL-PEG combinations [46].
Characteristic peaks of TZB were observed at 1651 cm− 1 and 1516 cm− 1 corresponding to a C = C bond, and 3355 cm− 1 correlated to NH stretching [62, 69]. These peaks are more clearly visible compared to those in TZHCL, in both the pure drug and in formulations with polymers, indicating good integration between the components. Similarly, characteristic peaks of the polymers mentioned before were present in the spectrum. Additionally, TZB-PCL-PEG pellet present a faintly shift of the peak at 1644 cm− 1. As it was mentioned before this suggests a non-covalent chemical interaction between the drug and the polymer.
Fig. 4
FT-IR spectra of drugs, polymers, and formulation pellets containing TZHCL (a-b), and TZB (c-d)
Power X-Ray diffractionXRD patterns of TZHCL and TZB pellets and the compounds alone are shown in Fig. 5. As we can observed in the figure the x-ray diffraction pattern of the pure drug and the excipients used in the formulation, exhibited reflection characteristic of crystalline systems. Some of the characteristic’s peaks of TZHCL could be seen at 11, 12, 25 and 32 degrees approximately (Fig. 5a). While for the two polymers used, PCL and PEG the characteristic peaks in their diffractogram showed values at 21 and 24 degrees, 19 and 23 degrees respectively. The existence of those peaks in the pellet formulations means that the drug has been well incorporated. The resulting pellets, however, exhibited a notable reduction in the intensity of the pure compounds’ reflection plans along with the loss of other distinct peaks. In the spectrum of TZHCL pellet containing PEG it was possible to observe a partial amorphization with some characteristic peaks belonging to the PEG. On the other hand, the sample without PEG, TZHCL-PCL pellet, present a marked decrease in the intensity of the reflection plans, and disappearance of some characteristic plans for both, the polymer, and the drug, was observed, indicating a partial amorphization of the drug in the system. On the other hand, also pellets containing TZB and the compounds alone exhibited characteristic peaks demonstrating their crystallinity (Fig. 5b). Peaks observed at 9, 11, 19, 28, and 29 degrees corresponded to TZB, while peaks at 21 and 24 degrees were related to PCL, and peaks at 19 and 23 degrees to PEG. The presence of these peaks in the prepared pellets indicates that TZB was thoroughly incorporated into the matrix system. However, there was a noticeable decrease in the intensity of the peaks in the pellet samples, and some peaks were not observable, this could suggest a partial amorphization of the formulation. These results align with the DSC spectrum of the drug demonstrating that the drug still crystalline.
Fig. 5
X-ray spectra of drug, polymers, and formulations, containing TZHCL (a), and TZB (b)
In vitro release study of tizanidine hydrochlorideThe release profiles of the pellets and implants containing TZHCL in combination with different compounds are presented in Fig. 6. Pellets developed by compression, pellets formulated by VCM, and both types of pellets with a PCL membrane were tested. All formulations evaluated were able to release more than 70% of the drug loaded in the implant device during the experiment period. Compressed tablets without the membrane were unable to maintain drug release for more than 1 day, unlike tablets produced by VCM. Pellets of TZHCL-PCL and TZHCL-PCL-PEG released the drug over 25 and 3 days respectively. Interestingly, pellets containing PVP and HPBCD presented faster releases than TZHCL pellets. HPBCD forms inclusion complexes with a wide variety of compounds while PVP has been extensively used to form polymer/drug complexes [70, 71]. Accordingly, these results are not surprising as these compounds will contribute to increase TZHCL dissolution rate. The direct compression method is widely used for manufacturing oral tablets [72, 73]. Therefore, it is a low cost and easy to scale manufacturing method. It has been reported for the manufacturing of subcutaneous implants for long-acting delivery of HIV drugs [74]. Our primary goal was to load the system with significant amounts of the drug to create a long-lasting implant. Unlike oral tablets, the need for excipients is less critical for this administration route, which made obtaining compressed pellets with short release challenging. On the other hand, VCM pellets are manufactured differently. In this case, mini tablets can be easily developed with the desired shape and homogeneity. The components are exposed to high temperatures until they melt together and create a matrix. The drug dispersed in a polymeric matrix slows down release, as the polymer needs to degrade to expose and release the drug. Although the VCM-pellet containing PCL showed the longest release, its duration is still not promising for a long-acting system device. Hence, a tubular membrane was included as part of the final implant device.
Implants comprising PVP, HPBCD, and the drug alone were inserted into the PCL tubular membrane, and it was observed that the release duration improved compared to pellets alone to 5, 11, and 25 days, respectively. In the case of implants with VCM tablets, the release duration also improved, reaching 80 days for the TZHCL-PCL implant and 19 days for the TZHCL-PCL-PEG implant. Clearly, the tubular membrane helps to control the release of TZ. Similar systems have been reported in the literature [34], but loaded with different drugs and formulation methods.
Fig. 6
Cumulative release of TZHCL pellets (a-b), TZB pellets (c), TZHCL implants (d-e), TZB implants presented in percentage of TZ released (f), and mg released per day from the TZHCL and TZB implants (g-i). All results shown as means +/- S.D., n = 4
The pellet formulated with TZB-PCL released the drug by 96 ± 10% over 150 days, whereas the pellet formulated with TZB-PCL-PEG delivered TZ at 94 ± 1% after 50 days. A nearly linear release profile was observed in the first 20 days for the formulation with both polymers, followed by a gradual decrease. Once again, the pellet containing PCL exhibited longer release compared to the formulation containing a mixture of PCL-PEG. These results are consistent with the absence of PEG, a water-soluble polymer, in the implants’ structure. PEG typically creates pores during the release process, aiding in drug delivery.
The surface of the pellets was analysed under SEM after the release study, revealing that the presence of PEG resulted in a more porous polymeric matrix (Fig. 1). This supports the theory that erosion influenced the drug release due to the water-soluble polymer in the matrix. Additionally, the pellets were evaluated in conjunction with the tubular membrane; in this scenario, the TZB-PCL formulation achieved 200 days, releasing 93 ± 5% of the drug, while TZB-PCL-PEG lasted 130 days, releasing 89 ± 7% of TZ. Clearly, the polymeric membrane helps to extend drug release compared to pellets alone. The formulation with PCL showed nearly linear release, maintaining a constant amount of TZ released per day throughout the experiment. Polymeric membranes have been previously employed to develop implant devices, demonstrating their capability to enhance drug delivery.
TZ in both forms, the salt and base, have been evaluated as a model drug for the formulation of an implantable long-acting drug delivery system to treat spasticity related to multiple sclerosis. Current treatments such as oral treatments can lead to systemic side effects like drowsiness, weakness, or gastrointestinal issues [75]. Intrathecal baclofen pumps are effective because they deliver the drug directly into the spinal fluid; however, their placement requires an invasive surgery with ongoing monitoring to avoid complications like infections or pump malfunctions [76]. These subcutaneous implants have distinct attributes over current treatments for spasticity in MS. They are small in size, have the capability to provide a less invasive treatment, and can offer sustained and localised drug delivery for long periods of time. This can lead to more consistent control of spasticity with fewer systemic side effects, as the drug bypasses the gastrointestinal tract, improving the adherence to treatment. Considering the low oral bioavailability of TZ, the formulated implants could be able to release amounts of drug between 0.2 and 3 mg per day which is a significant amount to treat a patient subcutaneously. Furthermore, the implants will not only improve the quality of life of the patient but will also reduce the burden in the health-care system, ameliorating the number of hospitalizations for relapses. Moreover, implants can be development with different drug loadings, shapes, and techniques to offer a more personalised treatment depend on the needs of the patient. Additionally, the maintenance require for subcutaneous implants is less compared to pumps, making them a more convenient option for some patients.
Regarding economic costs of MS, it has been reported that the cost of managing spasticity in MS patients increases with the severity of the condition [77]. Implants could be used early to help control spasticity progression. A UK study estimated that annual spasticity-related costs range from £217 in the early stages to £33,163 in later stages [77]. Early spasticity management has been proven to significantly reduce overall disease management costs [77]. Finally, patient perspectives on implantable devices for MS treatment have been previously evaluated, indicating a preference for this approach over conventional treatments due to the reduced risk of relapse [75]. The study also highlighted that patients would be willing to compromise some treatment efficacy in favour of switching from regular injections to a long-term implant [75].
Interestingly, alternative implants for spasticity treatment exist, such as intrathecal pumps for baclofen delivery [78]. These devices are w
Comments (0)