
Remember me
Seventy undergraduate students in the spring of 2024 were recruited for the primary analyses (2D group n = 33, 3D group n = 37). Preliminary data were collected across the 2023 calendar year (i.e., spring, summer, and fall 2023 semesters) and modifications in procedure and assessment helped to inform the current procedures. The 2023 data are treated as preliminary due to differences in procedure, issues with data contamination, and edits to assessment questions throughout 2023.
Participants were excluded if they were under 18 years old or not enrolled in an upper-level Human Gross Anatomy course. They received course credit for participation; extra credit and monetary incentives were not offered. After completing the assignments, students were given the opportunity to provide informed consent on whether their data could (or could not) be used in research analysis. Participants with data collection represented in the results are from the 2024 cohort. General demographics were collected, but specific demographics were not paired with experimental and observation data, as many marginalized identities (e.g., female, BIPOC [Black, Indigenous, People of Color]) were not adequately represented within the research team. Additionally, analysis related to cognitive load differences among demographic groups was not conducted on these groups to maintain anonymity of BIPOC students. The program has a small number of BIPOC students which would allow for identification. This study adhered to CSU Institutional Review Board policies and was approved under IRB #4132.
Study DesignThe research team used the mental rotation test scores to randomize participants into two homogeneous groups based on visuospatial ability. Students were divided into a group that participated in either the two-dimensional module or the three-dimensional module (2D n = 33; 3D n = 37). Before the start of the intervention, all participants completed a pre-test and a pre-survey to measure existing understanding of laryngeal anatomy. These pre assessments also captured student attitude and perception of VR in anatomy education, their prior use of VR and video games, and their overall physical comfort with using VR. Participants then watched a module covering the anatomy of the larynx using either 2D or 3D presentation depending on their experimental group. Both modules were viewed while in immersive VR. A post-test and post-survey were administered immediately following the viewing experience.
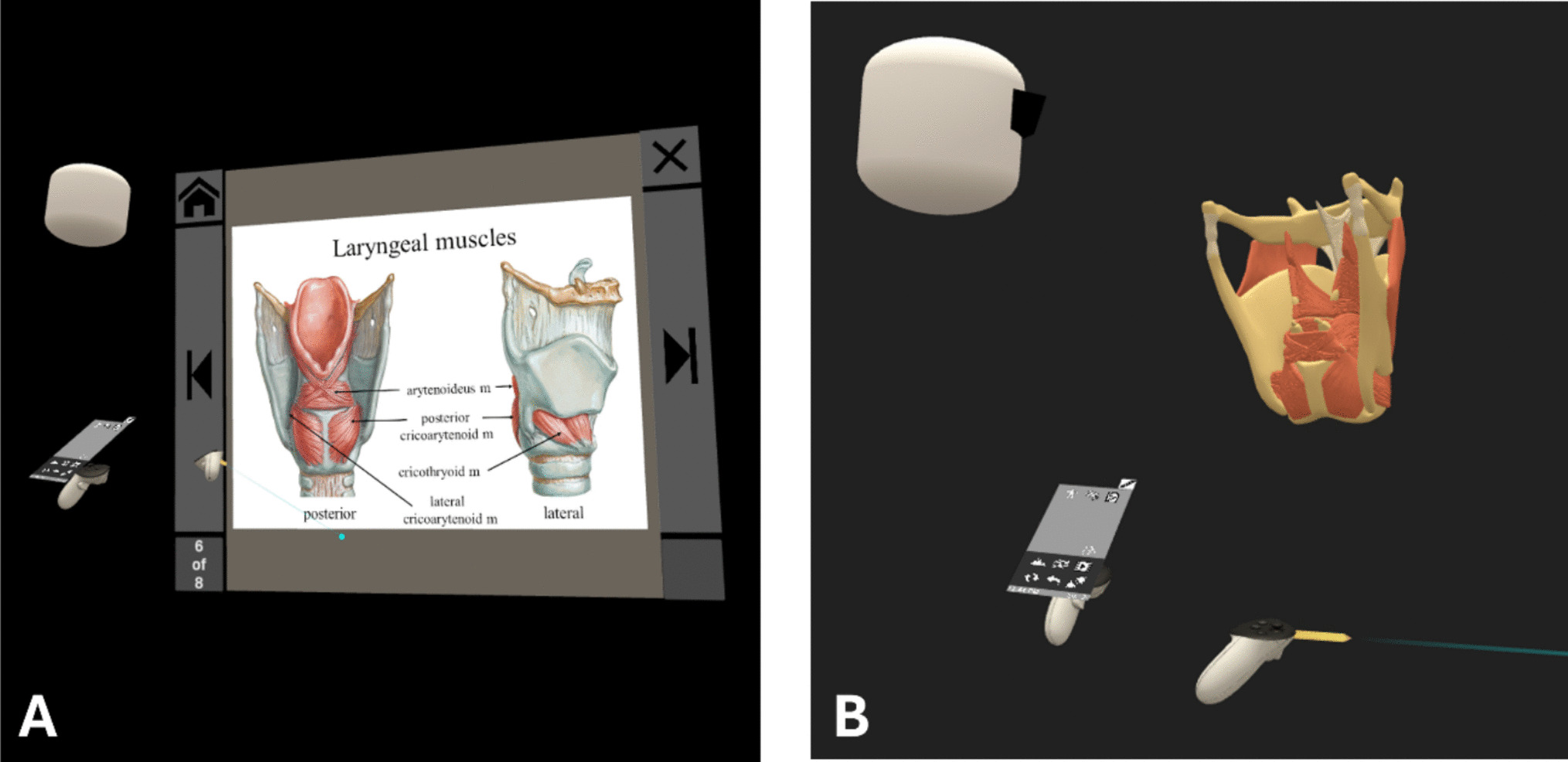
ModulesThe investigators utilized existing software (Perspectus VR) to build the two modules shown in VR. The 3D module and the 2D module were conducted in immersive VR. In both modules participants were asked to watch a pre-recorded lesson covering the anatomy of the larynx, a subject that was chosen for its structural complexity. Once in the fully immersive virtual environment, no controllers or model manipulation were used after the recording began. To ensure consistency, a senior instructor recorded both modules to maintain a similar outline, content, and verbiage. The duration of the 3D module was two minutes and four seconds, and the 2D module was two minutes and 45 s. Similarly, a concerted effort was made to keep the scripts in each module as close as possible. Keeping the modules to three minutes or less provided adequate time to review the relevant anatomical information, while limiting the risk of cognitive overload. Students were given the opportunity to watch the 3D or 2D module during VR open lab times, but they were not required to complete both modules. Students were tracked via a sign-up sheet and online survey to determine if they had completed at least one module. Some students watched both modules, but the second viewing was completed at a later time, after the post-test and post-survey were administered. Figure 1 shows what the participants saw during a similar moment in both the 2D and 3D modules. Table 1 describes the differences between the two modules.
Fig. 1
Participants’ view of analogous content in both the 2D and 3D modules. (A) In the 2D group, students saw the instructor navigate through a slide show with labeled images of the larynx. (B) In the 3D group, students viewed the instructor interact with a dynamic virtual model of the larynx; as the instructor interacted with the virtual model, text labels would appear naming the respective structure (not pictured here). In both images, the white avatar head depicts the senior instructor
Table 1 Differences between modulesTable 1 highlights the differences between the two modules.
Measuring Cognitive Load (aim 1)To examine aim 1, a virtual reality head mounted display (HMD) was used in this investigation: the HP G2 Reverb Omnicept edition. This headset contains biometric sensors to track eye movements (eye-tracking), pupil dilation (pupillometry), and heart rate variability (pulse plethysmography) which achieved ~ 79% accuracy in aligning quantitative cognitive load measures with qualitative reports [21]. The Omnicept reports a cognitive load score based on its algorithm and integrated software. This cognitive load score was collected as participants watched their respective module.
Student Attitude and Experience (aim 2)To examine aim 2, a pre-survey was used to examine student characteristics and experiences. The survey included questions about student attitudes toward VR in anatomy education, preference for using VR, physical comfort with VR, how frequently they used VR in the past, and if they played video games in the past (Table 2). Students were also asked if they were retaking the course at the time of the research study. Each survey was coded by two researchers using a deductive approach, categorizing responses into groups (e.g., positive, negative, mixed; comfortable, uncomfortable, mixed; likes VR, does not like VR, mixed feelings toward VR). Key-terms were established prior to initial coding. Codes were added and recategorized following initial coding before being used for a final assessment. Student responses that were unclear to both researchers were excluded from analyses. Table 2 demonstrates this process.
Table 2 Pre-survey questions and relevant study goalsStudent Perception of Cognitive Load (aim 2)Similarly, to examine how student experience affected cognitive load, we utilized a post-survey to capture student perception of cognitive load. We adapted the NASA task load index into a survey that, for each question, included an open-ended response as well as 10-point Likert scale [22]. This allowed students to quantitatively rate each of the questions and provide comments. Researchers coded the qualitative responses across six factors – physical demand, mental demand, temporal demand, perceived task difficulty, perceived success, and any negative emotions—as low (1), medium (2), or high (3). The NASA task load index is included as Supplemental Item 1.
Mental Rotation Test (aim 3)Visuospatial ability was assessed using the Mental Rotation Test (MRT) initially developed by Vandenberg and Kuse in 1978 [23]. The Mental Rotation Test presents participants with a target image next to four comparison images. Participants are tasked with correctly identifying the two rotated versions with the comparison set by marking them with an X. There are twenty-four questions that participants complete after a seven-minute instruction and demonstration period covering the mechanics of the test. Students were given three minutes to complete the first half of the assessment, followed by a two-minute quiet break, and then three minutes to complete the second half of the assessment. The MRT was given to participants prior to the pre-test and pre-survey to assess aim 3. Assessments were scored by two researchers; points were only given if the student identified both correct images. Researchers then used these data to assign students to research groups and to ensure similar visuospatial ability (as measured by the MRT) among the two groups. Researchers also used this data to explore the relationship between visuospatial ability and cognitive load (aim 3).
Comments (0)