
Remember me


Full population demographics and baseline characteristics, including sex, race and ethnicity, can be found in the primary articles for each of the ONWARDS 1–5 trials [5,6,7,8,9]. Overall, participant baseline characteristics and demographics were numerically similar between icodec and once-daily insulin comparator groups in ONWARDS 1–5 [5,6,7,8,9].
In previously insulin-naive participants, 10.3–13.6% of hypoglycaemia alert values and 9.6–18.9% of clinically significant or severe hypoglycaemic episodes were attributed to physical activity in the icodec arms across ONWARDS 1, 3 and 5, while 10.8–16.3% and 6.6–8.6%, respectively, were attributed to physical activity in the once-daily insulin comparator arms of these trials (Fig. 1). In insulin-experienced participants, 13.1–22.6% of hypoglycaemia alert values and 9.7–19.1% of clinically significant or severe hypoglycaemic episodes across ONWARDS 2 and 4 were attributed to physical activity in the icodec arms, while 19.0–20.6% and 19.8–31.0%, respectively, were attributed to physical activity in the once-daily insulin comparator arms (Fig. 1).
Fig. 1
Proportion of hypoglycaemic episodes that were attributed to physical activity during the on-treatment period of ONWARDS 1–5. The on-treatment period was defined as the onset date on or after the first dose of the trial product and no later than the first date of either the follow-up visit, the last date on trial product +5 weeks for once-daily insulin and +6 weeks for once-weekly insulin, or the end date for the in-trial period (defined as the time from randomisation to whichever occurred first of the last direct participant–site contact, withdrawal of informed consent, the last participant–investigator contact before loss to follow-up, or death). Hypoglycaemia alert value was defined as a blood glucose value <3.9 mmol/l but ≥3.0 mmol/l, confirmed by a blood glucose meter; clinically significant hypoglycaemia was defined as a blood glucose value <3.0 mmol/l, confirmed by a blood glucose meter; severe hypoglycaemia was defined as hypoglycaemia with severe cognitive impairment requiring external assistance for recovery. aThe choice of the once-daily insulin analogue (insulin degludec, insulin glargine U100 or insulin glargine U300) was made at the discretion of the investigator. Aspart, insulin aspart; degludec, insulin degludec; glargine U100, insulin glargine U100; glargine U300, insulin glargine U300; icodec, insulin icodec; OD, once-daily
Across all trials, there were no consistent differences in the proportions of physical activity-attributed hypoglycaemic episodes with icodec vs the once-daily insulin comparators (Fig. 1). These episodes were mainly alert value or clinically significant hypoglycaemia, with one physical activity-attributed severe hypoglycaemic episode reported in the icodec arm of ONWARDS 1 (Fig. 1), which had other possible contributing factors reported, such as diet change.
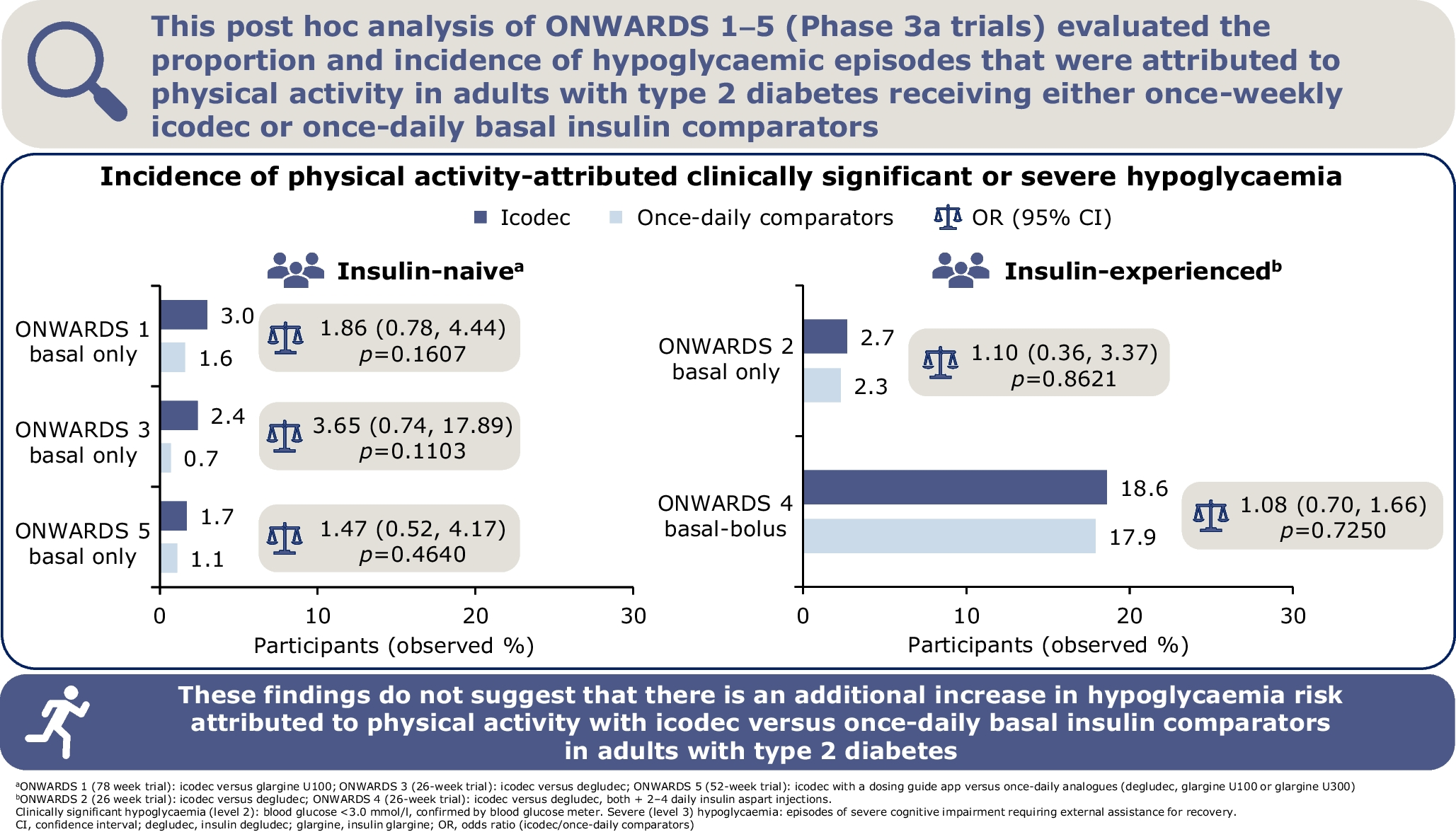
In both insulin-naive and insulin-experienced participants, the incidence of physical activity-attributed clinically significant or severe hypoglycaemic episodes was consistently ≤3.0% in ONWARDS 1–3 and 5. In ONWARDS 4, the incidence was numerically higher in both treatment groups (icodec vs insulin glargine U100: 18.6% vs 17.9%), which was expected given the basal-bolus insulin regimen used in this trial (Fig. 2).
Fig. 2
Observed incidence of physical activity-attributed clinically significant or severe hypoglycaemia with icodec vs once-daily insulin comparators during the on-treatment period of ONWARDS 1–5. The table presents the number of participants in each treatment arm that were included in the analyses that are presented in the bar graph. The on-treatment period was defined as the onset date on or after the first dose of trial product and no later than the first date of either the follow-up visit, the last date on trial product +5 weeks for once-daily insulin and +6 weeks for once-weekly insulin, or the end date for the in-trial period (defined as the time from randomisation to whichever occurred first of the last direct participant–site contact, withdrawal of informed consent, the last participant–investigator contact before loss to follow-up, or death). The incidence of hypoglycaemia was analysed using a binary logistic regression model, with treatment, geographical region, sulfonylurea/glinide use (ONWARDS 3) and personal continuous glucose monitoring device use (ONWARDS 2 and 4) as fixed factors. Missing data were imputed using multiple imputations. Clinically significant hypoglycaemia was defined as a blood glucose value <3.0 mmol/l, confirmed by a blood glucose meter; severe hypoglycaemia was defined as hypoglycaemia with severe cognitive impairment requiring external assistance for recovery. ORs (icodec/once-daily insulin comparator) are shown; there were no statistically significant differences between treatment arms in each trial (two-sided p values for the test of no treatment difference [with no correction for multiplicity] were p=0.1607, p=0.1103 and p=0.4640 for ONWARDS 1, ONWARDS 3 and ONWARDS 5, respectively, and p=0.8621 and p=0.7250 for ONWARDS 2 and ONWARDS 4, respectively). aThe choice of the once-daily insulin analogue (degludec, glargine U100 or glargine U300) was made at the discretion of the investigator. Aspart, insulin aspart; degludec, insulin degludec; glargine U100, insulin glargine U100; glargine U300, insulin glargine U300; icodec, insulin icodec; OD, once-daily
Across all trials, there were no statistically significant differences in the odds of experiencing a physical activity-attributed clinically significant or severe hypoglycaemic episode with icodec vs once-daily insulin comparators (Fig. 2).
The frequency of recurrent clinically significant or severe hypoglycaemic episodes in the 24 h after a physical activity-attributed clinically significant or severe hypoglycaemic episode was low, with no such episodes being reported in ONWARDS 1, 3 and 5. In ONWARDS 2 and 4, this frequency was numerically higher with icodec vs the once-daily insulin comparator; no additional severe episodes were reported in any participants across the trials (ESM Table 3).
Comments (0)