In this cross-sectional study involving 1796 samples, we found a significant positive correlation between LAP and EAA. Importantly, there is a nonlinear relationship between LAP and EAA (P = 0.034); the LAP inflection point is 41.12, with an OR of 0.96 before the inflection point and an OR of 1.11 after, showing a 15.6% increase in OR after the inflection point. After adjusting for relevant covariates, the regression results showed that higher LAP was associated with an increased likelihood of EAA; compared with the first quartile (Q1) of LAP, the fourth quartile (Q4) had a 77% increased risk of EAA, with an odds ratio of 1.77. There was a significant difference between the two, and the fully adjusted model had an AUC of 0.706. In terms of population attribution, the regression analysis of the adjusted model showed that the population attributable fraction was 41.6% for age stratification, 10.4% for LAP, 8.5% for gender, 4.0% for smoking, and 3.5% for marital status. These findings align with previous research, suggesting that LAP is an independent influencing factor for EAA [27,28,29,30,31, 41].
In the subgroup analysis, we found that the correlation between LAP and EAA was stronger in people over 60 years old compared to those under 60, with an OR increase of 10% and P < 0.001. In terms of gender, females had a higher OR than males, with a 7% increased probability of EAA in females compared to males.
Obesity is a major global public health issue, and LAP is a reliable, simple, and effective indicator of obesity [14, 15, 27,28,29,30,31,32,33,34,35,36]. EAA represents the biological aging of the human body, with DNA methylation playing a crucial role. EAA is closely associated with tumors, endocrine metabolism, cardiovascular diseases, etc., and HorvathAge is a key indicator for evaluating EAA [6,7,8,9,10,11,12,13,14,15]. There is a close relationship between obesity and EAA, as obesity accelerates biological aging [19,20,21,22, 27,28,29,30,31]. This study marks the first exploration of the relationship between LAP and EAA, specifically in relation to HorvathAge.
However, the potential mechanisms between LAP and EAA remain to be studied, and the following explanations are possible. LAP is a reliable indicator of obesity and is closely related to visceral obesity [32,33,34,35,36]. In obese populations, the expansion of white adipose tissue and the resulting local hypoxia lead to abnormal secretion functions in adipose tissue. Inflammatory-related adipokines are abnormally secreted, activating immune cells (particularly monocytes and lymphocytes). The release of pro-inflammatory cytokines mediated by immune cells interferes with insulin signaling pathways, causing insulin resistance, which then affects blood glucose and the endocrine system. The abnormal secretion of adipokines causes low-grade chronic inflammation, stimulating the formation of TNF-α and IL-6, which inhibits the action of adiponectin, affecting insulin secretion, anti-inflammatory responses, and cardiac function [23,24,25,26,27,28,29]. Additionally, the decline in insulin receptors on hypertrophic adipocytes reduces insulin effectiveness, while the increase in peripheral free fatty acids in obese individuals can damage peripheral tissues and decrease insulin utilization. All of these factors contribute to increased production of reactive oxygen species, leading to oxidative stress [23,24,25,26,27,28,29, 41,42,43].
Oxidative stress is a major pathogenic factor in obesity-related comorbidities, causing insulin resistance in peripheral tissues and is closely related to endocrine diseases such as diabetes. Prolonged oxidative stress can damage the blood–brain barrier, accelerating neurodegenerative changes in the brain. Oxidative stress impairs cardiovascular function, leading to an increased incidence of cardiovascular disease. It also damages mitochondrial function, resulting in a range of diseases, particularly tumors [28, 29].
Insulin resistance, low-grade chronic inflammation, and impaired immune function are characteristics of obesity as well as aging, which is particularly evident in the elderly [25,26,27,28,29,30,31]. In the subgroup analysis of this study, the OR for EAA increased by 10% in elderly individuals over 60 compared to those under 60, which further supports this conclusion. Various measures to reduce the lipid accumulation product (LAP) can improve epigenetic age acceleration (EAA), studies have shown that weight loss, smoking cessation, and a healthy diet can effectively reduce EAA [2, 44].
Advantages and limitations
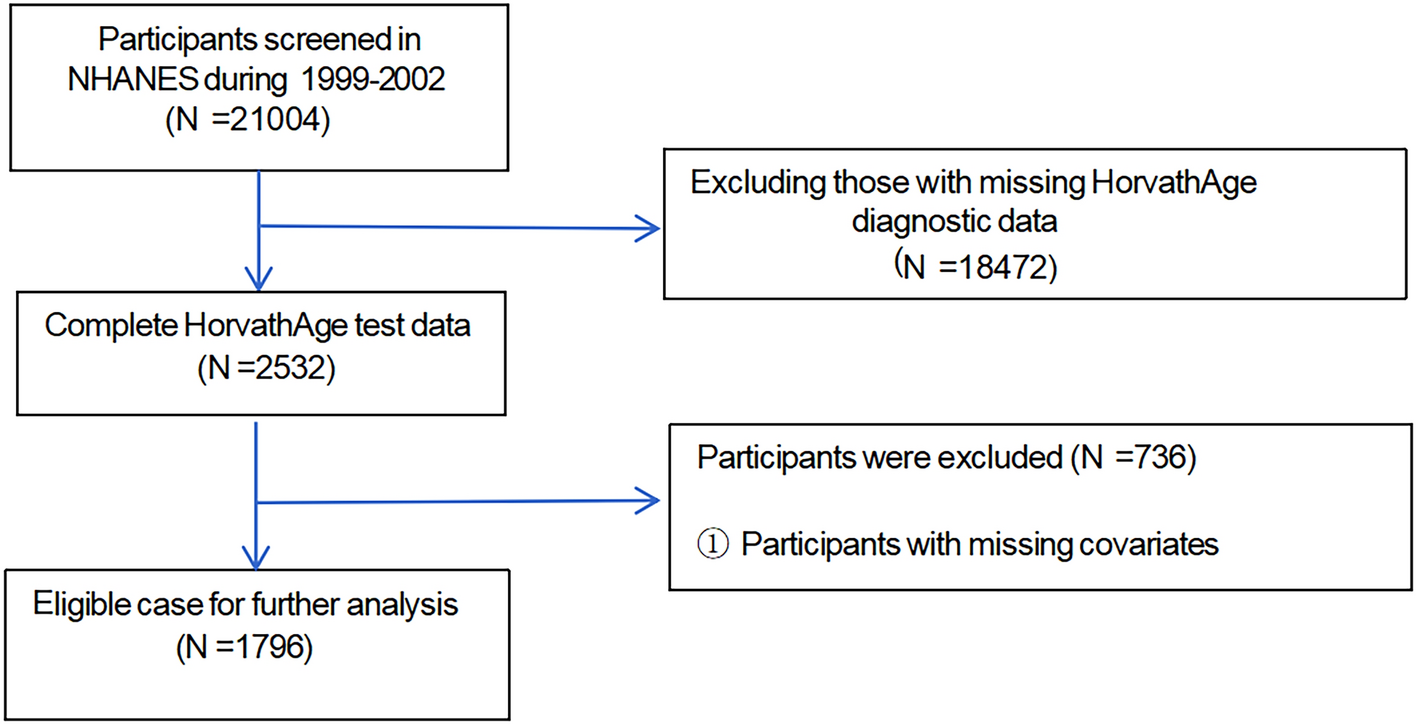
Specifically, this study has the following advantages. First, our research is based on NHANES data, which offers the advantage of a large sample size. In addition, we adjusted for relevant covariates and conducted subgroup analysis and propensity score matching, making the results of this study robust and reliable.
However, this study still has some limitations. Firstly, although we adjusted for covariates as thoroughly as possible, there may be uncontrolled factors; however, the model’s AUC after adjusting for all covariates was 0.706, indicating that our study still has good clinical significance. Secondly, our study population was limited to American adults over 50. Therefore, additional studies are required to assess if these findings can be extrapolated to other nations.


Comments (0)