Study design and cohort
This retrospective cohort study included patients with asthma who participated in a pay-for-performance program promoted by the National Health Insurance Administration (NHIA) of Taiwan to optimize medical care [15]. The NHIA pay-for-performance asthma program encouraged medical institutions to join the initiative to strengthen tracking management and health education for asthma patients. Patients were eligible to participate in the program only if they were diagnosed with asthma and had that diagnosis reconfirmed by the same doctor at the same clinic or hospital within 90 days. Additionally, it was stipulated that the doctor explain the purpose of the treatment plan to the patients and ask for their cooperation with regular return visits and follow-ups.
The asthma education program was conducted and asthma medication was provided in accordance with established guidelines in Taiwan. In fact, the Taiwan Society of Pulmonary and Critical Care Medicine supervised the training certification classes to improve the skills and knowledge of physicians and case managers. Certified physicians and case managers provided in-person training pertaining to asthma control, asthma care planning and proper inhaler usage. The outcomes were regularly monitored by the NHIA.
The asthma patients in this study were referred to our tertiary facility from other medical institutions due to poor asthma control, making it difficult to define the date of asthma diagnosis. Thus, the index date was defined as the date of patient enrollment in the pay-for-performance program, while the baseline period was defined as the 1-year period prior to the index date.
Asthma was confirmed by pulmonologists on the basis of respiratory symptoms, pulmonary function tests and treatment responsiveness. Following the confirmation of the initial diagnosis, the patients were monitored at intervals of 3 months for at least 1 year. The NHIA implemented the aforementioned program in eligible medical centers across Taiwan. This study included patients with asthma who attended at least two clinical visits within 90 days of diagnosis at Chang Gung Memorial Hospital, Linkou Branch. Enrollment in the program was voluntary and patients signed a consent form [16].
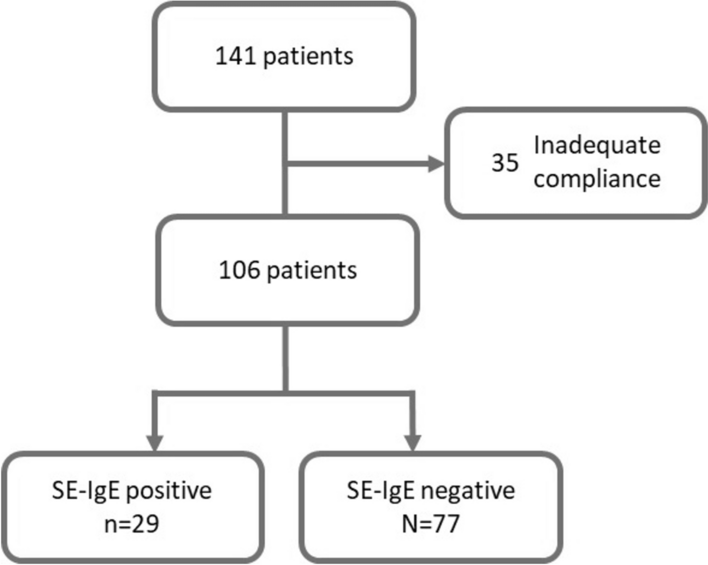
All patients underwent an SE-specific IgE test conducted using the ImmunoCAP system (Phadia, Uppsala, Sweden) at our hospital between January and August 2021. Patients without a diagnosis of asthma (International Classification of Diseases, Tenth Revision code: J45), those with coexisting chronic obstructive pulmonary disease and those exhibiting medical non-compliance were excluded. Adequate compliance was defined as adherence to scheduled clinical visits and the use of > 80% of prescribed medications, as verified by self-reported data [17]. The study protocol was approved by the Institutional Review Board of Chang Gung Memorial Hospital (permit number: 202400365B0).
Data and definitions
We retrospectively analyzed the following patient characteristics and parameters: age at SE-specific IgE measurement, sex, smoking status, body mass index, AE events in the previous year, pulmonary function test results, asthma control test (ACT) scores and type 2 inflammatory biomarkers (e.g., total IgE level, eosinophil cation protein level, eosinophil count and specific IgE level [ImmunoCAP]). A specific IgE value of > 0.35 kU/L was considered a positive test. We evaluated sensitization to four SEs (SEA, SEB, SEC, and toxic shock staphylococcal toxin). SE sensitization was defined as having sensitization to at least one SE. The incidence of AE events was compiled from patient medical records and self-reported data, where AE was defined as a decline in forced expiratory volume in 1 s (FEV1) to < 60% of personal best necessitating an oral corticosteroid burst as well as an unscheduled clinic or emergency room (ER) visit or hospitalization. In addition, we recorded the baseline incidence of ER visits and asthma-related hospitalizations within 1 year prior to recruitment and during the follow-up period.
Definition of fungal sensitization
Fungal sensitization was confirmed by a positive reaction in the IgE antibody test against specific fungi, defined as one or more positive results among four types of fungi, according to the diagnostic criteria proposed by Agarwal et al. [18]. The fungal allergens in this panel included Penicillium chrysogenum, Cladosporium herbarum, Aspergillus fumigatus and Alternaria alternata. An IgE level of ≥ 0.35 kU/L was considered positive.
Outcome measurement
This study included 106 patients who were stratified into two groups based on the presence of SE-specific IgE antibodies: SE-IgE+ group (those with SE sensitization) and SE-IgE− group (those without SE sensitization). Spirometry was performed in accordance with guidelines issued by the American Thoracic Society and European Respiratory Society. This involved recording data on FEV1 (% predicted), forced vital capacity (FVC) and the FEV1/FVC ratio. Treatment outcomes were evaluated in terms of ACT scores, pulmonary function test results and AE events.
Statistical analysis
All data are presented as mean ± standard deviation or frequency and percentage values. Categorical variables were analyzed using the Chi-squared test and continuous variables were analyzed using the Student’s t-test. Post-treatment changes in pulmonary function were evaluated using a paired-sample t-test. Statistical analysis was performed using SPSS (version 26; IBM Corporation, Armonk, NY, USA). Significance was set at p < 0.05.


Comments (0)