
Remember me
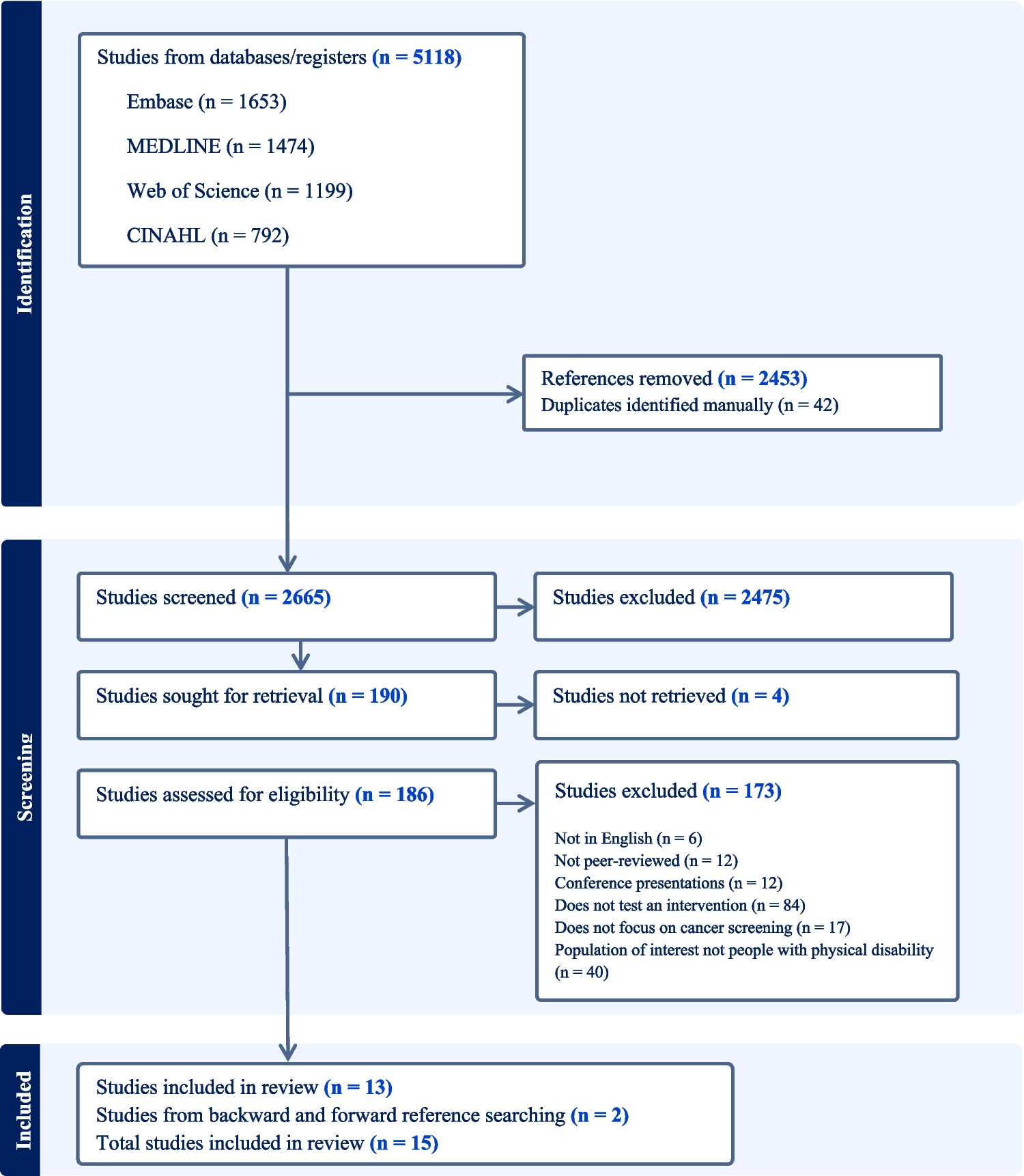
The search identified 2,665 records. After abstract and title screening, 186 studies were assessed for eligibility; 13 studies were eligible for the review. Two additional studies were added after backward and forward reference searching, giving a total of 15 studies included in the final review (Fig. 1).
Fig. 1
PRISMA flow diagram of literature search [16]
Study CharacteristicsThe country, study design, cancer type, population, intervention, primary outcome, and results are included in Tables 1 and 2. The included studies were published between 1995 and 2022 and were conducted in the United States (n = 13), Turkey (n = 1), and Saudi Arabia (n = 1). The populations of people with disability included people in the D/deaf community (n = 10), people with physical disability (n = 4), and one study that included people with physical, hearing, vision, and/or cognitive disability (n = 1). The studies evaluated screening interventions for breast cancer (n = 7), cervical cancer (n = 3), colorectal cancer (n = 1) and a combination of breast, cervical and/or colorectal cancer (n = 4). Twelve studies used quantitative methods, and three studies used mixed methods. Across studies, interventions targeted key stages of the cancer screening behavior change process [23, 24] including improving knowledge and awareness, supporting intention formation, and reducing practical and environmental barriers to screening participation.
Table 1 Characteristics of included studiesTable 2 Results of the interventionsEducational InterventionsThe reviewed studies primarily examined educational interventions (13/15) with a focus on increasing knowledge, an important determinant of behavior change. Few studies examined the effect on cancer screening intention or participation, with intention outcomes limited by the well-documented intention-behavior gap.
Educational interventions for the d/Deaf community included workshops [25,26,27] with additional materials [27], videos [28,29,30,31,32] and humor-infused messages [33]. The workshops were delivered in American Sign Language (ASL) by interpreters [25] or community leaders [26] or in Turkish Sign Language by health professionals [27]. The videos [28,29,30,31,32] utilized sign language (ASL or TSL), voice-over and captions, with some incorporating graphics [28, 29, 32]. The humor infused messages comprised 12 cancer messages, each paired with a joke submitted by members of the d/Deaf community, signed in ASL with English subtitles [33]. Workshops increased knowledge of cervical [25, 27] and breast cancer screening [26], with knowledge retention ranging from immediate [26] to two months [25], or three months post-intervention [27]. The videos increased knowledge of cervical [32], breast [29] and colorectal [31] cancer screening immediately post intervention to two months post intervention. One video reported no improvement in cancer prevention [30] and the multimodal intervention, video delivered in a workshop, did not show a clear significant increase in knowledge but did increase intention to screen [28]. The humor infused cancer messages increased knowledge immediately post intervention and one week post intervention [33].
Educational interventions for people with physical disability included, workshops [34], the ‘Right to Know’ campaign [35] and home-based patient navigation [36]. The workshop was delivered by people with physical disability and included six months of telephone support [35]. The campaign provided information to the public about accessibility of mammography centers and center staff with educational materials [36]. The home-based patient navigation, led by a nurse-midwife, provided information about cancer risk factors and helped participants schedule a mammogram appointment [24]. The workshop increased Pap screening in the intervention group, but there was no increase in mammography uptake. There was also no effect on self-efficacy, perceived susceptibility, perceived benefits and screening intention [35], important antecedents to participating in screening according to the Health Belief Model [37]. The pilot study of the home-based patient navigation demonstrated an increase in adherence to mammography screening but only included 11 women [24]. The campaign reported an increase in the percentage of centers considered to be totally accessible from 22.5% in 2009 to 52.5% in 2015 [36].
One study included participants with a range of disabilities, including physical, hearing, vision, and/or cognitive disability [25]. The intervention consisted of an interactive workshop with optional one-on-one coaching. The workshop incorporated multiple communication modes, including ASL, large print materials and braille resources. They reported an increase in breast cancer knowledge and higher likelihood of participants scheduling a breast cancer screening exam and/or mammography.
Environmental InterventionsTwo studies examined environmental interventions focused on adapting health care facilities to increase screening participation [38, 39]. Facility adaptations for breast cancer screening in people with spinal cord injury involved the introduction of physically accessible examination tables, transfer lift equipment, and longer appointments. Staff also received training in disability awareness, sensitivity, and relevant skills [38]. Facility adaptations for the d/Deaf community focused on providing full-time sign language interpreters and reducing health costs in the primary care center [39]. Adapting the health care facility for people with physical disability did not significantly increase patients' willingness to receive mammograms or perform breast self-examinations [38]. Adapting the health care facility for the d/Deaf community was associated with increased participation in mammography and Pap screening, but not breast self-examinations [39].
Quality AssessmentQuality assessment found study risk of bias was high in many of the studies due to methodological issues (Appendix 2). Most studies were prospective, quasi-experimental using a pre-post evaluation and one was a retrospective observational study which relied on self-report of screening behavior [39]. Study sample size varied (n = 11 – 299) [36, 40]. Risk of bias concerns included high attrition [30, 40]; difference in demographic characteristics between groups [39] and another cluster randomized by location [27]. Given the low number of studies found, all were included in the review.
Comments (0)