
Remember me
The impact of the Kin KeeperSM educational intervention on first and appropriately timed breast and cervical cancer screening (primary outcome) and functional cancer literacy over time (secondary outcome) at the individual and family level were evaluated using a two-arm longitudinal RCT (NCT01910350) among Black, Latina, and Arab women in Detroit and Dearborn, Michigan. To achieve the primary outcome measures of breast and cervical cancer screenings, we conducted longitudinal monitoring of women at 12, 18, 24, 30, and 36 months post home-based educational intervention for both arms. Details of the study design and methods have been reported elsewhere [34]. Briefly, the design was based on the following principals: (1) employing the community-based participatory structure of the Kin KeeperSM educational intervention model; (2) testing the intervention with scientific rigor; (3) building longstanding community-university research collaborations [35]. To that end, we engaged our community partners using a community-based participatory approach to design the protocol. Medically underserved women participating in a community-based health program delivered by CHWs were invited to participate in the cancer prevention intervention addressing literacy and screening with other women in their families to test the effects of the Kin KeeperSM educational intervention compared with a control group. Data were collected from 2011 to 2015, and ongoing analyses specific to the randomized controlled trial were conducted in 2012 and 2015. The Michigan State University IRB approved the research protocols.
Study PopulationParticipants were recruited from the Detroit Health Department and ACCESS in Dearborn, Michigan. Our partnering health clinics utilize CHWs in many programs. CHWs had an average case load of more than 30 women. Working with their supervisors, they recommended the CHWs from non-cancer programs. Following, the CHW was able to approach her client about participating in the research project. Trained female CHWs recruited women from their caseloads. Three participant groups included CHWs, their clients (kin keepers in the intervention, participant clients in the control), and clients’ female family members. CHWs had to be Black, Latina, or Arab (bilingual for Latina and Arab), age ≥ 21, trained as CHWs with at least 5 years of experience, affiliated with a public health program, and have completed 16 hours of Kin KeeperSM training. Following the CHW’s training regarding our research, she was able to approach her client about participating in the research project. Each CHW recruited 14 women, allowing for attrition. Details regarding the recruitment process have been reported previously [36].
Client eligibility were (1) age ≥ 21–70; (2) self-identified as Black, Latina, or Arab; (3) participated in a public health program that utilized a CHW; and (4) agreement to assemble her adult female family for home visits and assist in locating them for follow-ups. The family eligibility criteria were: (1) related to the client as either their client’s mother, grandmother, daughter, sister or aunt; (2) women age ≥ 21–70; (3) self-identified as Black, Latina or Arab and (4) at least two of those family members should be age 40–64 (and eligible for Breast and Cervical Cancer Control Program (BCCCP), which was the criteria at the time of data collection). Prior screening history and cancer history were not considerations for inclusion or exclusion. The home of the client was the setting for the intervention.
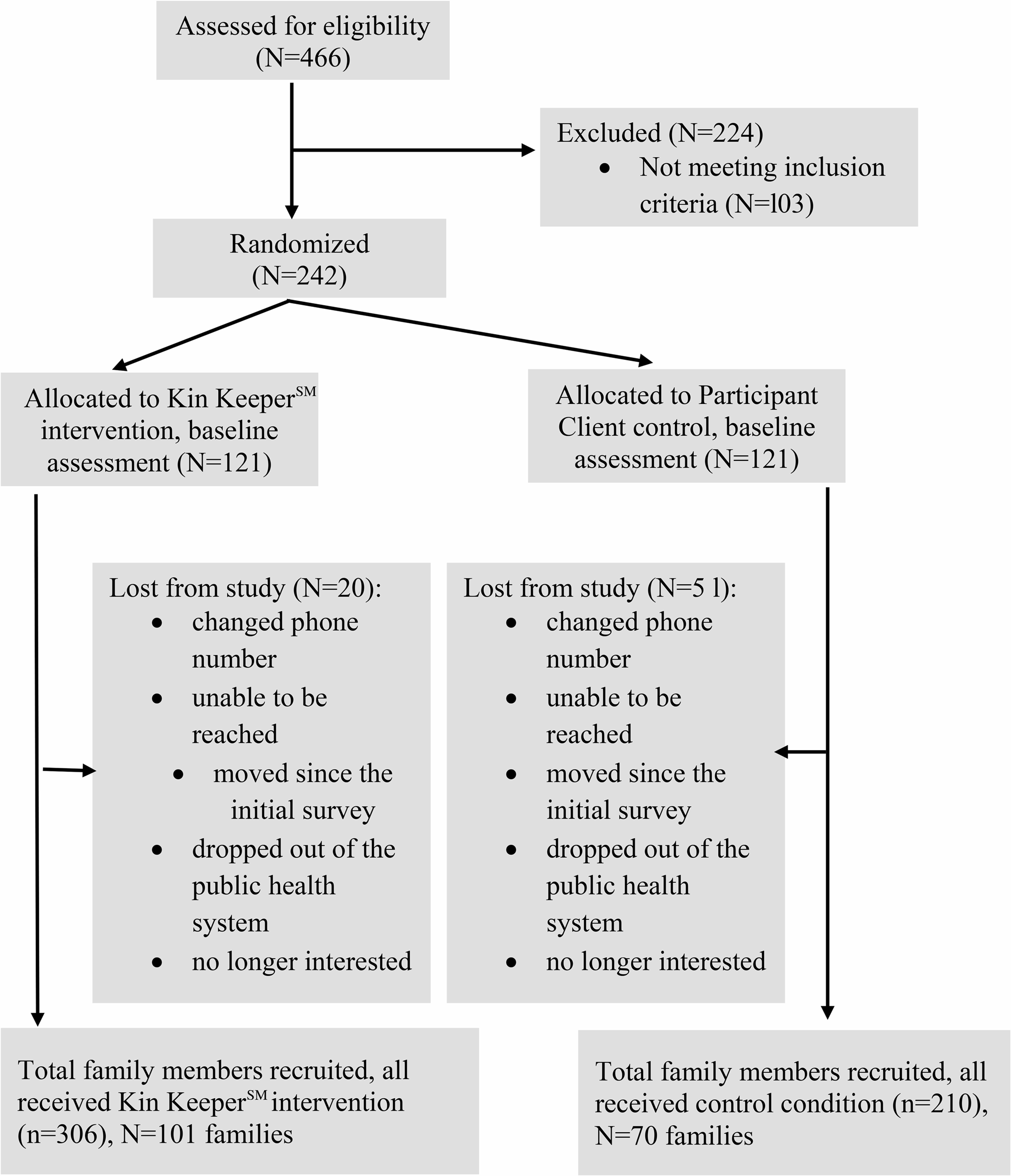
InterventionRandomization took place at the level of clients served by an individual CHW. After confirmation of study eligibility, written informed consent, and completion of baseline data, participants were randomized to either the intervention or control group based on proximity in age. Age was used as a stratification variable to increase the equivalence of the treatment and comparison groups on a variable of potential relevance to the study outcomes. Then, a computer generated one of two possible, equal probability outcomes to assign one member of the pair to the intervention group and the other to the control group. From this process, the kin keeper educational intervention and the control arms were each assigned 121 women who, in turn, were tasked to recruit their family members. Twenty Kin KeeperSM women were lost from the study, and fifty-one from the control arm. With family sizes varying from 3 to 5; 306 women received the Kin KeeperSM educational intervention while 210 women were assigned to the control arm. Even with loss to follow-up, we have adequate power (at least 80% power) to detect an increase of 15–20% points in screening proportion between the intervention and comparison group. The power/sample size calculation assumed an estimate of proportion for the screening proportion (e.g., receipt of time-appropriate mammogram) ranging from 0.35 to 0.55 in the control group. It also assumed a modest intra-cluster (within family) association of ρ = 0.10, and a two-sided 5% significance test. Figure 1 displays the CONSORT diagram.
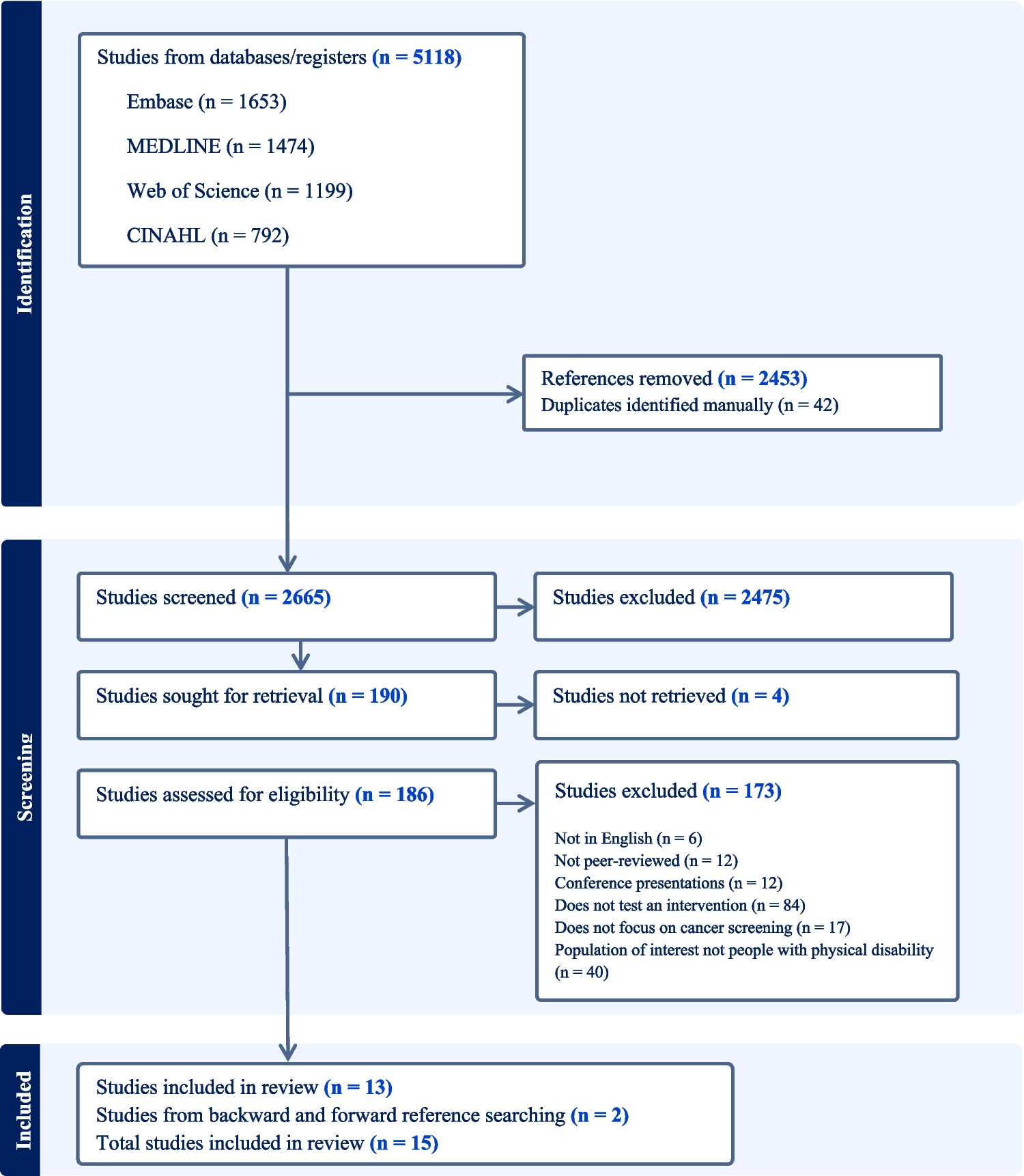
Fig. 1
CONSORT flow chart. Note: N is the number of keen keepers/control client participants representing each family, and n is the total number of family members, including the Kin Keepers or the Participant Client controls
CHWs invited their clients to participate in the study. Once deemed eligible, the CHW read the informed consent and the sociodemographic form while participants followed along independently, completing a baseline questionnaire. Following randomization, the CHW contacted the kin keeper and the participant client to schedule the first of two family face-to-face educational home visits. The kin keeper invited 3–4 adult female family members to her home to receive the educational intervention, yielding a maximum of five individuals, including the kin keeper. The same procedure was used for the comparison group that included the participant client and her family. The control group received written information only.
The first home visit focused on breast health and wellness. Family members completed the informed consent and a baseline sociodemographic questionnaire, identical with the questionnaire answered by the index participants. As part of the protocol, informed consent and the questionnaire were administered orally. All participants (family and kin keeper) took the pre-intervention Breast Cancer Literacy Assessment Tool (Breast-CLAT) [29]. Participants (family members and kin keeper) were able to select their first language. Following the education intervention, the Breast-CLAT was administered again. The second family visit was scheduled on-site during the first family visit, with all the family members in attendance. The second home visit focused on cervical cancer prevention. CHWs opened the session by asking for questions or concerns about the previous breast cancer home visit. Participants followed the protocol of completing the Cervical Cancer Literacy Assessment Tool (C-CLAT) [30]. Both educational home visits took place in the evenings or weekends between June 2010 - March 2011 and lasted between 1.5 and 2.0 h each.
MeasuresParticipants (kin keeper and family) completed a baseline questionnaire that included sociodemographic characteristics and family medical history (i.e., cancer, health co-morbidities, behavioral risk factors, access to health services, and exposure to cancer prevention information). The primary outcome measure of breast and cervical cancer screenings was conducted at 12, 18, 24, 30, and 36 months post their home-based educational intervention using a self-report Personal Action Plan. The CHW individually administered this check-off-style form that enabled participants to set individual, age-appropriate goals. Personal action plans were completed at every follow-up session.
The secondary outcome measure, functional cancer literacy, was measured using the validated health literacy assessment tools: Breast-CLAT and C-CLAT [29, 30]. All instruments were culturally and linguistically translated, and Latina and Arab CHWs were bilingual; all participants (family members and kin keepers) were able to select their first language. The Breast-CLAT, a validated 35-item assessment, has three domains: awareness, knowledge, and screening and prevention that are in sync with the education intervention. The C-CLAT, a content-validated assessment, has 24-items with three domains: awareness, knowledge, and prevention and control. The Breast-CLAT and C-CLAT served as pre and post intervention measures during the home visits and for follow-ups at 12, 18, 24, 30, and 36 months.
Statistical AnalysisDescriptive statistics, treating each woman participant as the unit of analysis, were generated for baseline variables for both study arms. Basic inferential analyses that account for the family clustering were conducted to examine distributional differences in baseline characteristics between the two study arms. Longitudinal data analyses using a generalized estimating equations (GEE) technique were conducted to evaluate the Kin KeeperSM educational intervention effects on the primary and secondary endpoints. Specifically, for binary endpoints (e.g., providing a correct answer to a Breast-CLAT and C-CLAT question), logistic regression models coupled with a GEE estimation technique were used to describe the longitudinal profiles across time. The basic starting model imposed no linear structure on the time effects, but rather treated time as a categorical variable. The intervention effect was then evaluated using a Wald test of the interaction term between the time variable indicators and the study exposure indicator. Because the endpoints are binary, these interaction terms, when exponentiated, represent the ratio (kin keeper versus control) of longitudinal odds ratios comparing the follow-up to the baseline visits. Further analyses were conducted to describe a potential heterogeneity of the Kin KeeperSM educational intervention effect across the racial groups. These analyses helped determine if there are race categories that attenuate or accentuate the effects of the Kin KeeperSM educational intervention on primary and secondary endpoints. Consequently, the basic longitudinal model was extended to include three-way interactions involving Race, Intervention group, and Time.
Two primary causal inference analyses were conducted: one that treats the family as the unit of the analysis and the other that treats the individual women participants as the unit. The causal intervention effect under the family-level analysis was estimated without any confounder adjustment, due to the randomization being conducted at the level of clients served by individual CHWs. For individual-level analyses, however, the evaluation of the causal intervention effects on study participants’ outcomes presents a challenge due to the non-random assignment of individual participants to the two intervention arms, albeit a random assignment of kin keepers and participant clients to the two study groups. For this reason, causal inference techniques that control for observed confounders as a source of potential biases were considered. Specifically, a balancing strategy based on propensity scores (PS) was used to mitigate potential differences at baseline among individual participants in the two study groups [35,36,37,38]. The PS scores were used to obtain an unbiased estimate of the average treatment effect of the intervention on the primary and secondary study endpoints. These scores were generated using an elaborated (parametric) logistic model for a woman participant’s probability to receive the Kin KeeperSM educational intervention that includes baseline characteristics and functions thereof (e.g., interactions, and higher order terms such as squares). Variables used to generate the PS estimates were selected among the baseline characteristics, taking into account existing knowledge of breast and cervical cancer literacy and screening behaviors. Specifically, they include variables such as age, race, education level, prior exposure to breast and cervical cancer literacy and knowledge, family history of cancer, type of insurance, and marital status. The full list of potential confounders used in this propensity scoring model is provided in the supplementary material.
Results of the family-level analysis are presented in the manuscript due to its potential to control both measured and unmeasured confounders and a relatively large number of families being randomized. Individual-level PS analysis results and further details of the statistical analysis are in the supplementary material. All analyses were performed with the use of SAS software, version 9.4 (SAS Institute).
ResultsBaseline characteristics of the overall sample (n = 516) stratified by intervention group are summarized in Table 1. Baseline characteristics are well balanced between the two groups, with none of the p-values exceeding 5%.
Table 1 Sample size distribution (Cell counts and relative frequencies - in parenthesis) of Sociodemographic Characteristics at Baseline stratified by GroupOverall, the Kin KeeperSM educational intervention significantly improves the odds of correctly answering Breast-CLAT and C-CLAT questions from baseline compared to the control arm (Breast-CLAT p-value = 0.0007 and C-CLAT p-value < 0.0001). For either literacy score, the greatest improvement of the kin keeper arm occurred between the baseline and the immediate post-visit. During this time frame, the Kin KeeperSM intervention arm improved its odds of correctly answering a Breast-CLAT question by 2.4 times (p-value < 0.0001) compared to 1.61 (p-value < 0.0001) for the control arm, resulting in a ratio of longitudinal ORs of 1.49 (p-value = 0.0007). Likewise, the kin keeper arm improved its odds of correctly answering a C-CLAT question by 2.41 times (p-value < 0.0001) compared to the control arm of 1.43 (p-value < 0.0001 during the same time frame, resulting in a ratio of longitudinal ORs of 1.68 (p-value < 0.0001). We note, however, that the Kin KeeperSM arm experienced a significant decrease in the odds of correctly answering Breast-CLAT or C-CLAT questions between the immediate post-visit and the one-year follow-up visit (Breast-CLAT p-value = 0.0016 and C-CLAT p-value = 0.0060). This is in contrast with the control arm, whose odds remain constant from the immediate post-visit to the 36-month follow-up (Breast-CLAT p-value = 0.7964 and C-CLAT p-value = 0.8626). By the 36-month follow-up, the significant decrease noticed for both Breast-CLAT and C-CLAT between immediate post-visit and one-year follow-up in the Kin KeeperSM arm increased over time and returned to similar immediate post-visit significance, respectively. Estimates of the proportions of correctly answered Breast-CLAT and C-CLAT questions across study visits for each intervention group are plotted. Similar results were found with individual-level analyses using the propensity scoring method (Tables 1 and 2).
Table 2 Estimates, Standard Errors (in parentheses) and P-values of Longitudinal Odds Ratios for Correctly Answering Breast-CLAT Questions Stratified by Group, and their ratiosFurther analyses indicated that the differences in literacy across time are mostly driven by Black American study participants and Latinas. No difference in literacy profiles for Arab women (Table 3).
Table 3 Estimates, Standard Errors (in parentheses) and P-values of Longitudinal Odds Ratios for Correctly Answering C-CLAT Questions Stratified by Group, and their ratiosLongitudinal Analyses of Breast and Cervical Cancer Screening BehaviorsTable 4 shows that the odds of receiving a clinical breast exam, mammogram, and PAP exam significantly improved for both groups. The Kin KeeperSM educational intervention does not significantly improve the odds of receiving a clinical breast exam and mammogram exam at 12, 24, and 36 months from baseline compared to the control arm (CBE p = 0.9400; MAM p = 0.7787). The Kin KeeperSM educational intervention also does not appear to significantly improve the odds of receiving a PAP screening at 36 months from baseline compared to the control arm (p-value = 0.3865). Estimates of the group-specific proportions of CBE, mammogram, and Pap screenings across time are presented in Figs. 2 and 3.
Table 4 Estimates, Standard Errors (in parentheses) and P-valuand P-values of Longitudinal Odds Ratios for Correctly Answering C-CLAT Questions Stratified by Group, and their ratios of Longitudinal Odds Ratios Evaluating the Trends for Receiving Clinical Breast Exam, Mammography and PAP Smear Stratified by Group, and their ratiosFig. 2
Estimated proportions of MAM screenings with accompanying confidence intervals for the two study arms. Note: The temporal changes in the proportions of MAM screenings do not significantly differ between the two comparison groups across time; consistent with parallel profiles across time
Fig. 3
Estimated Proportions of PAP screenings with accompanying confidence intervals for the two study arms. Note: The temporal changes in the proportions of PAP screenings do not significantly differ between the two comparison groups across time
Additional analyses were conducted to evaluate the effect of the Kin KeeperSM educational intervention on the first-year screening behaviors of the subgroup of women who never received a screening exam at enrollment. Among these women, there was no significant difference between the Kin KeeperSM educational intervention group and the control group on the odds of receiving the first CBE at one-year follow-up (p-value = 0.3629). Among eligible women who never had a mammogram at enrollment, there was no significant difference between the Kin KeeperSM educational intervention and the control group on the odds of mammogram behavior at one-year follow-up (p-value = 0.1564). Because no intervention effect was found on screening behaviors, analyses by racial subgroups were not conducted. Finally, similar results were found with individual-level analyses using the propensity scoring method (Table 3).
Comments (0)