
Remember me
Participants included health care providers (n = 18; physicians, nurse practitioners, physician assistants) and stakeholders (n = 6; professional organizations, health departments, community clinics), reflecting a comprehensive range of perspectives on the HPV Decide tool’s implementation. Participants were between 26 and 64 years of age, with a majority being female. They were predominantly non-Hispanic White. The specialties represented include OB/GYN, Family Medicine, and other fields like Oncology and Public Health. Health care providers in the sample had an average of 14 years in practice (range: 11 to 22) and worked predominantly in community clinics, although others worked in private practices, outpatient clinics, and academic settings.
Feedback on HPV DecideFive main categories emerged through the qualitative data analysis. These categories characterize issues related to (1) the preferred method of delivery, (2) timing of tool utilization, (3) needed support and training, (4) barriers to implementation, and (5) facilitators to implementation.
Preferred Methods of Delivery. Health care providers expressed a preference for electronic delivery mechanisms for the decision aid tool, emphasizing ease of access and modern technology integration. The majority favored the use of QR codes, which patients could easily scan with their smartphones in the waiting room or during office visits.
“In the exam room. In the waiting room, too. Both places would definitely work to give them access to it if it was just as simple as scanning a QR code, because most people have smartphones these days.” (P24, Physician, Family Medicine).
However, recognizing the diverse needs of their patient population, some providers also highlighted the necessity of having physical pamphlets available, especially for those without access to smart devices.
“I think some offices will still need a printable version or a paper version. So I can always make that version because some offices do a lot of screening while people are in the waiting room.” (P10, Nurse Practitioner, OB/GYN).
Timing of Tool Utilization. Regarding the timing of when the tool should be used, there was a consensus towards utilizing it before the patient-provider interaction. Providers believed that engaging with the tool in the waiting room could help patients prepare better for their consultation, potentially enhancing the discussion on preventive health measures such as vaccinations.
“Yeah, I think the best place that I would want to see this used would be before the patient even reaches the provider. So, something in the waiting room.” (P01, Physician, Family Medicine).
This pre-consultation usage was seen as a way to inform providers about any hesitations or questions the patient might have, thereby making the actual consultation more efficient and focused.
Provider Support and Training Needs. Providers were mixed in their views on the need for specific training to implement the decision aid tool effectively. Some argued for a brief, targeted training session that would familiarize all clinical staff with the tool’s functionality and purpose.
“I think if it were being introduced into the clinical practice, we’d want to have a team meeting or a clinician’s meeting.” (P09, Physician, Family Medicine).
Conversely, other providers felt the tool was intuitive enough that extensive training would not be necessary, though they stressed the importance of ensuring that all staff were aware of the tool’s existence and basic operation.
Barriers to Implementation. Time constraints emerged as the most significant barrier to the implementation of the decision aid tool, with providers concerned about the potential for extended patient wait times. Technological issues, such as unreliable Wi-Fi and integration challenges with existing electronic health records (EHR), were also noted as significant obstacles.
“Internet access, WiFi in the office… You know what I mean? It just won’t load, I would say would be the biggest thing practically that I can think of.” (P12, Physician, OB/GYN).
Facilitators for Implementation. To facilitate the adoption of the decision aid tool, providers suggested integration with electronic health records, enabling seamless access during clinical encounters. The idea of including prompts or alerts for unvaccinated patients was favored as a way to remind health care staff to discuss the HPV vaccine. Providers also recommended using patient portals to disseminate the tool.
“Let’s say some people have clinics where they might send an email or patient portal that clinics have and send the link out to anybody who’s interested…if you have people that are connected to a patient portal where they get things prior to their appointments or a little notification, ‘Are you interested in learning more about HPV vaccination?’ That are sent out.” (P20, Physician, OB/GYN).
Overall, health care providers recognized the potential of the decision aid tool to enhance patient education and streamline clinical interactions, albeit noting several logistical and technological challenges that would need to be addressed to maximize its effectiveness and ease of use in diverse clinical settings.
Phase 2: Quantitative ResultsCharacteristics of the study sample (N = 600 health care providers) are reported in Table 1. On average, respondents were 56.1 years of age (SD = 9.3). The majority were male (64.5%) and White (66.7%). On average, providers had 24.1 years of practice experience (SD = 8.2). Most practiced in suburban areas (60.7%), with fewer in urban (27.2%) and rural (12.2%) settings. The sample was evenly distributed across three disciplines: OB/GYN, Family Medicine, and Internal Medicine (each 33.3%). About a quarter (24.5%) worked in Federally Qualified Health Centers, 33.5% were affiliated with academic/teaching organizations, and 43.3% were part of larger healthcare networks. Additionally, 66.7% were in private practice.
Table 1 Sample characteristics of exploratory sequential mixed methods studyThe overall likelihood of adopting this tool was high, with 68.3% of providers likely to use it, indicating strong potential for integration into clinical practice (Table 2). Almost half of providers (46.5%) favored clinic-based access, whereas others suggested that patients should access the tool online on their own. Among those who favored clinic-based access, most providers selected the waiting room (29.0%) and pre-visit timing (27.6%) as ideal for tool use, emphasizing the need for integrating the tool into patient wait times and in preparation for an appointment. The preferred method of delivery was via the patient portal (34.8%), reflecting a preference towards leveraging digital platforms for patient engagement. Notably, doctors (99.0%), nurses (91.5%), and pharmacists (71.2%) were identified as the most appropriate personnel to facilitate the tool’s usage, but other provider types endorsed as facilitators included community health workers, medical assistants, and dentists.
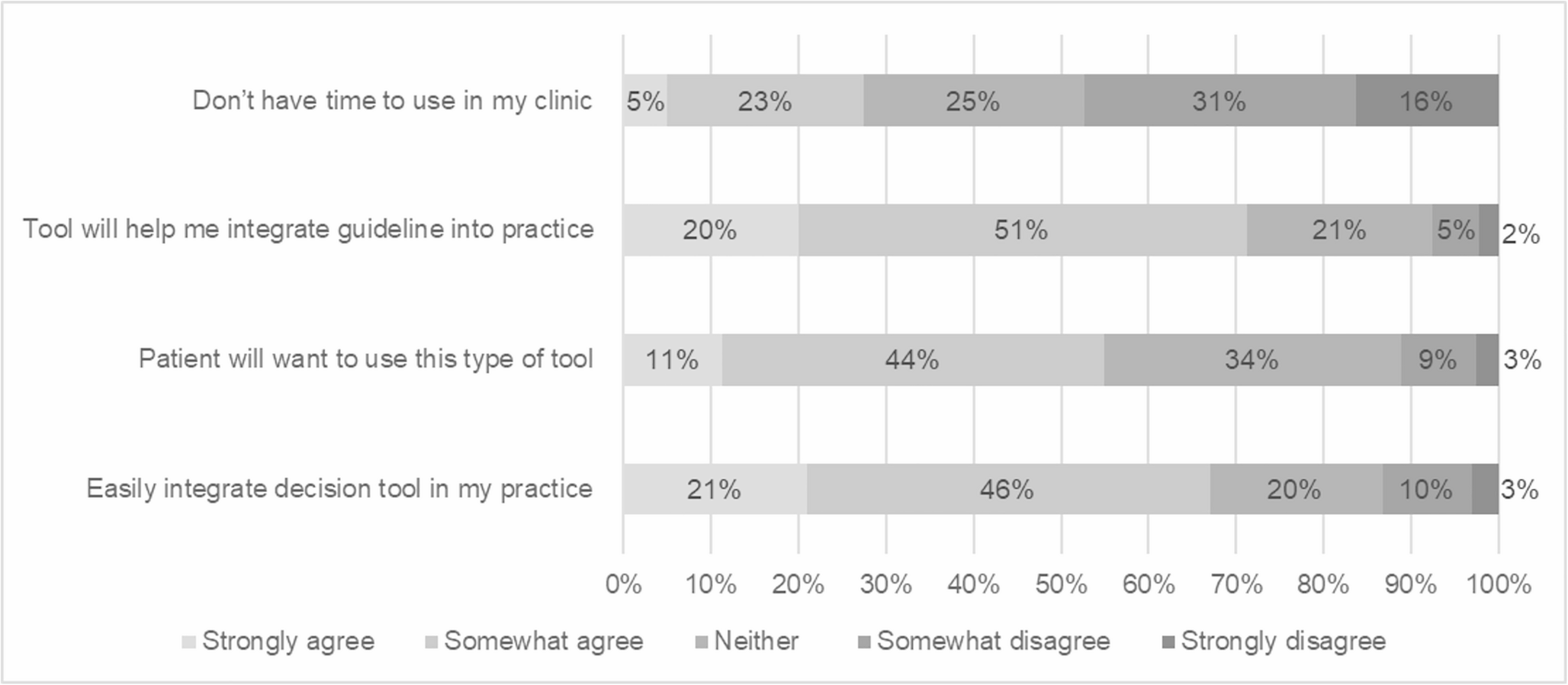
Table 2 Physician perceptions of the HPV Decide tool (N = 600)Most providers (67.0%) agreed that the tool could be easily integrated into their practice, and a majority (54.0%) believed that patients would want to use this type of tool (Fig. 1). Even stronger agreement (71.3%) was found for the statement that the tool would help integrate SCDM guidelines into practice. However, when considering time constraints, responses were mixed with 27.3% indicating that they might not have enough time to use the tool in their clinic, reflecting concerns about the practicality of its implementation in clinical settings (Fig. 1). These results suggest overall positive attitudes towards the HPV Decide tool, tempered by realistic assessments of time limitations in clinical environments.
Fig. 1
Physician beliefs about implementing the HPV Decide tool (n = 600)
Comments (0)