
Remember me
A user-centered, stepwise development process guided by the IRLM as conceptual framework was applied to tailor content and format to end-user needs, translating clinical recommendations into scalable, accessible self care interventions. The project team (AT, SB, LZ, CC, CH, JB, CW) defined the IRLM determinants, implementation strategies, mechanisms, and outcomes in a planning meeting.
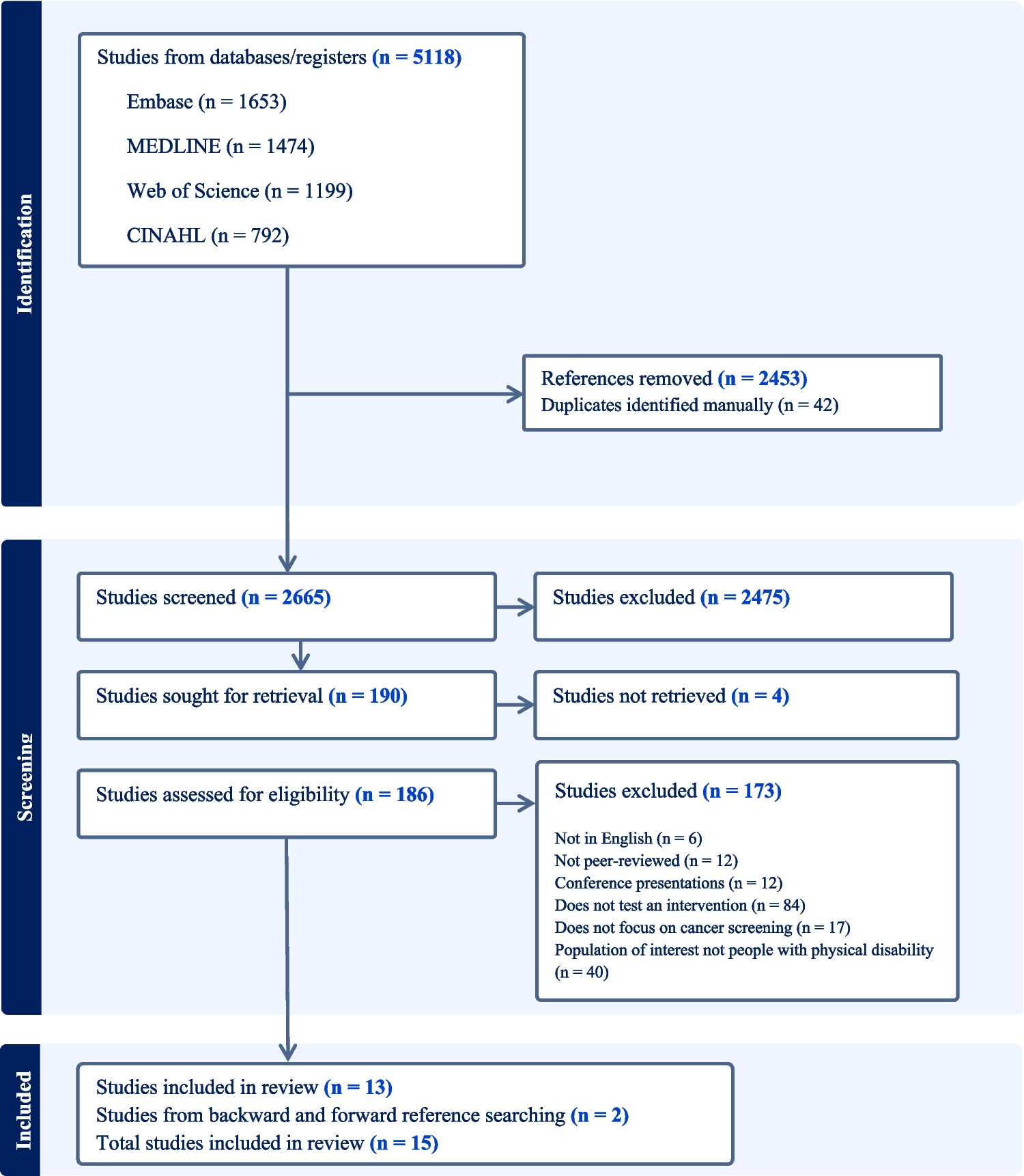
A participatory, mixed-methods design involved key stakeholders throughout the development of the online trainings (Fig. 1): MBM practitioners, experts, and health professionals contributed clinical knowledge, cancer patients represented end-user perspectives, and teaching experts supported didactic design. Stakeholders were recruited through purposive sampling [13].
Fig. 1
Digital training development process and stakeholder involvement
The Stakeholder Advisory Board included representatives from the relevant stakeholder groups (2 patients, 1 researcher, 1 oncologist, 1 clinical nurse specialist) and played an integral role in the development and decision-making.
Focus groups (2–8 participants; in-person or online) were used to explore knowledge, to understand opinions, and to obtain meaningful feedback. Sessions were moderated by a project team member following an interview guideline and were audio- or video-recorded.
Online surveys assessed post-training learning experience of participants covering navigation (5 questions), instructions (10), content (6) and applicability (1), and were answered using a 5-point numeric rating scale (1 = strongly disagree to 5 = strongly agree). Questions regarding navigation on the online platform were only included in patients’ questionnaire. Open-ended questions captured additional feedback.
Self Care TechniquesFor CRF acupressure, the expert group (LZ, TM, CW) suggested the acupressure points Yin tang, Anmian, Heart 7, Spleen 6, and Liver 3 as reported by [14]. For sleep problems, the same expert group developed a standardized schema based on the available evidence containing the acupressure points Du 20, Anmian, Heart 7, and Spleen 6 [4, 15,16,17]. Yin tang and Du 20 were stimulated unilaterally, the remaining points bilaterally.
As MBT, the exercise “3-minutes breathing space” [18] was selected by an expert group (ZM, CH, CW, NL). It guides a shift in awareness in three steps: (1) present-moment awareness, (2) focused breathing, (3) expanded body awareness. The instructions were adapted with expert and patient input. The final version was validated regarding understandability and applicability as on-site exercise with former cancer patients (N = 8) who evaluated their experience on a numeric rating scale (1 = strongly disagree to 6 = strongly agree).
Digital Training Development ProcessTwo separate digital trainings were developed through an iterative process for both self care techniques, with learning objectives aligned with the overall project aim.
First, relevant content was identified through focus groups with MBM-practitioners experienced in both self care techniques (N = 8). Second, in focus groups, technique-specific experts (acupressure: N = 3; MBT: N = 4) reached consensus on all key content components. Then, teaching experts (N = 3) defined instructional and assessment formats.
Trainings were iteratively piloted on an eLearning platform and revised three times with cancer patients. Subsequent testing of the trainings involved students of different health professions (N = 6), clinical specialists in the fields of medicine, psychology and other health-related disciplines (N = 17) and oncology-specialized nurses (N = 24), serving as proxies for patient perspectives.
The testing by health professionals included a validation of the acupressure instructions. Upon completion of the digital training for acupressure clinical specialists (N = 15) and oncology-specialized nurses (N = 24) were asked to demonstrate self-administered acupressure for each acupressure point in onsite sessions. One of three acupuncturists validated the correct self-administration (point localization, pressure intensity, postural control and respiratory coordination) using a scoring system with maximum scores of 12 or 14 for 4 or 5 acupressure points, respectively.
Finally, cancer patients (N = 7, with different cancer types) evaluated the final versions of the digital trainings.
eLearning PlatformThe digital trainings were delivered via the Open Learning Management System (Open LMS), where participants accessed them through email-based accounts. Online surveys were integrated into the platform alongside the trainings.
Data AnalysisFocus group data were analyzed using a rapid qualitative evaluation approach [19]. This approach involved iterative cycles of analysis conducted collaboratively by the research team in close interaction with stakeholders. The process integrated direct feedback from the focus groups with structured consensus-building discussions within the research team and between the research team and stakeholders. Analytical decisions and adaptations were documented in a transparent and systematic manner throughout the process [19].
Quantitative survey data were analyzed using IBM SPSS Statistics, Version 29.0.0.0, with means and standard deviations reported. Open-ended questions were summarized and discussed within the project team.
Ethical Approval and Consent to ParticipateThis study was conducted according to the national guidelines and regulations for research with humans. The Cantonal Ethics Committee Zurich waived the need for ethics approval (BASEC-No Req-2021–01499). Surveys were irrevocably anonymous and voluntary. Informed consent was obtained from all participants.
Comments (0)