
Remember me
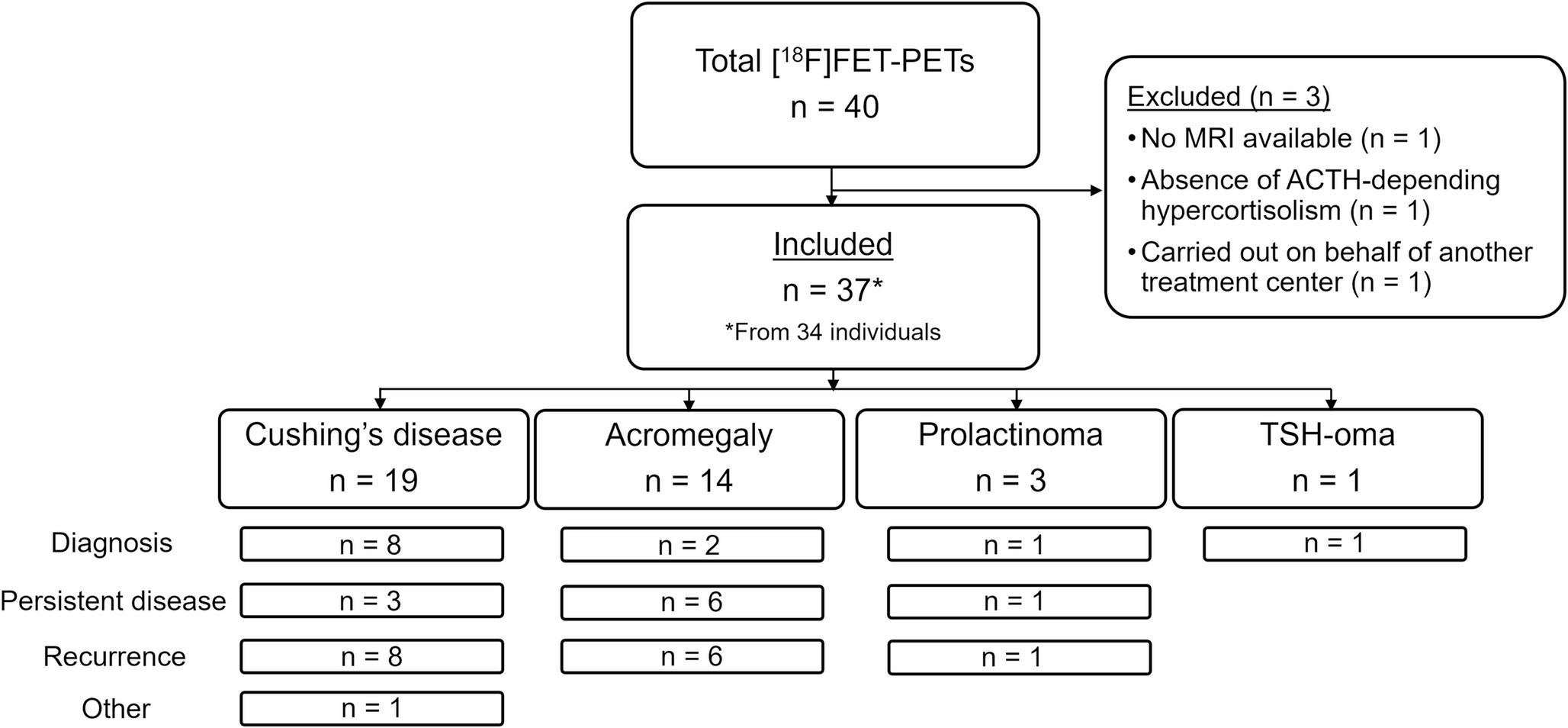
Forty pituitary [18F]FET-PETs from 37 individuals were conducted between January 2022/April 2025. Three [18F]FET-PETs were excluded: no MRI (n = 1), ACTH-independent hypercortisolism (n = 1), and request of [18F]FET-PET by another treatment center (n = 1). In total, 37 [18F]FET-PETs from 34 individuals with (suspected) CD (n = 19), acromegaly (n = 14), prolactinoma (n = 3), or TSH-oma (n = 1) were included, with a median follow-up duration of 1.0 year [0.6–1.8] (Fig. 1; Table 2). Median age at time of [18F]FET-PET was 45 years [35–58] and 68% of the scans were from females.
Fig. 1
Flowchart of included [18F]FET-PETs
Table 2 Characteristics of the cases per [18F]FET-PETThe [18F]FET-PETs were made during the diagnostic stage (n = 12), persistent disease (n = 10), recurrence (n = 14), and other (n = 1; suspected Nelson’s syndrome). MRI showed no visible lesion (n = 9), suspected microadenoma (n = 21), macroadenoma (n = 3), or multiple lesions (n = 4). Previous confirmative histopathology was present in the majority of [18F]FET-PETs of persistent disease or recurrence (CD: 73%, acromegaly: 83%, and prolactinoma: 100%). See supplemental Table 2 for detailed scan information.
Indication for [18F]FET-PETThe indications for [18F]FET-PETs were to identify and localize an adenoma that was not seen on previous MRIs (n = 8), to confirm increased tracer uptake of suspected microadenoma during diagnosis (n = 7), of which 5 were smaller than 6 mm in CD, to confirm increased tracer uptake of a remnant (n = 5), to discriminate between active remnants and postoperative changes (n = 11), and to localize the (most) active lesion out of multiple lesions seen on MRI (n = 4). In one scan, the additional indication was to identify a possible second adenoma due to discrepant histopathological results of the previous surgery (gonadotroph adenoma in clinical acromegaly; #25). In one patient with suspected Nelson’s syndrome, [18F]FET-PET was made to assess stereotactic radiotherapy as treatment option (#19).
Results of [18F]FET-PET co-registered/correlated with MRI[18F]FET-PET identified a single lesion in 28 scans (76%), two lesions in 1 scan (3%), and no lesion in 8 scans (22%) (Supplemental Table 2). Median SUVmax and LBR in the positive [18F]FET-PETs was 2.8 [2.4–3.1] and 2.9 [2.4–3.2], respectively (Table 3). SUVmax of lesions was higher than the SUVmax of the left and right cavernous sinus in 20 scans (71%). Overall, the Likelihood-scale was 5 in 15 (41%) scans, 4 in 4 (11%) scans, 3 in 8 (22%) scans 2 in 2 (5%) scans, and 1 in 8 (22%) scans. Semi-quantitative measures and Likelihood-scale did not differ between the PET/CT scanners in positive [18F]FET-PETs (Supplemental Table 3).
Table 3 SUV and Likelihood-scales of positive [18F]FET-PETs[18F]FET-PET localized a lesion in 8 (89%) of the cases with a negative MRI. Positive [18F]FET-PETs were concordant with MRI in 14/29 scans, and discordant (different location) in 2/29 scans. [18F]FET-PET was partly concordant with MRI in five scans, where MRI showed possibly multiple lesions and [18F]FET-PET at least one but not all of these lesions in 4 scans, while [18F]FET-PET showed possibly multiple lesions and MRI at least one but not all of these lesions in 1 scan. A suggestive lesion on MRI followed by a negative [18F]FET-PET was seen in seven scans. In one case, the positive [18F]FET-PET location (Likelihood-scale 2) was concordant with a structure on MRI interpreted as an intercavernous sinus (#21). Co-registration with MRI to improve anatomical correlation was possible in 76% of the positive [18F]FET-PETs and 38% of the negative [18F]FET-PETs. In the surgical cohort, co-registration with MRI was performed in 75%.
Multidisciplinary team meeting and proposed treatment strategiesAll but five [18F]FET-PETs have been discussed during the MDT meeting. Surgery was recommended 17 times. Of these cases, 14 [18F]FET-PETs showed a visible lesion (concordant positive: n = 9, partly concordant: n = 1, discordant MRI-/[18F]FET-PET+: n = 4). Despite a negative [18F]FET-PET, the MDT was convinced of a pituitary origin of hormonal hypersecretion in three cases, and exploratory endoscopic surgery was offered (#2, 16, and 20).
Shared decision making between surgery and continuation of medication was recommended five times. The MDT advised against surgery 7 times. Continuation of medication was advised twice, once in a MRI-/[18F]FET-PET + patient due to cavernous sinus invasion (#32) and in another patient with MRI+/[18F]FET-PET- (#33). Shared decision making between continuation of medication with or without radiotherapy was offered to a patient after his second [18F]FET-PET (#25), as re-resection after the first positive [18F]FET-PET did not result in confirmative histopathology nor remission, and uptake seen on the second [18F]FET-PET showed potential cavernous sinus involvement.
A wait-and-scan strategy was advised in 3 cases: one of recurrent CD with MRI+/[18F]FET-PET- (#17), the case with suspected Nelson’s syndrome as no visible target lesion for radiotherapy was seen on MRI despite positive [18F]FET-PET (#19), and a case of recurrent acromegaly and increasing IGF-1 levels but normal OGTT (#31).
Clinical performance of [18F]FET-PETFull surgical cohortIn total, 20 surgeries were performed (CD: 16/19, acromegaly 3/14, prolactinoma 1/3, TSH-oma: 0/1) (Table 4, Supplemental Table 4). Surgery was performed after 17 positive and 3 negative [18F]FET-PETs. Exemplar scans are shown in Fig. 2. One patient received surgery twice, once after every [18F]FET-PET (#11 and 14). The other two patients that underwent two [18F]FET-PETs were only surgically treated after their first [18F]FET-PET (#13 and 23). Suspected adenoma tissue was identified intraoperatively by neurosurgeons in all cases. In surgeries performed after positive [18F]FET-PETs the adenoma was located at the location of [18F]FET uptake in 88% and more lateral in the other two cases.
Fig. 2
MRI co-registered/correlated with [18F]FET-PET images. Scan 2: Female patient in the diagnostic stage of Cushing’s disease (CD) with a lesion suspected for a microadenoma on conventional (a) coronal T1, (b) coronal T2 and (c) sagittal T1 post-contrast MRI. (d) [18F]FET-PET-CT image showed no focal uptake. Co-registration of (e) coronal, (f) sagittal, and (g) transversal [18F]FET-PET with (h) reconstructed 3D T1 coronal MPRAGE, (i) sagittal MPRAGE, and (j) reconstructed transversal MRPAGE. The patient underwent a TSS targeted at the lesion seen on MRI, which was located during surgery and suspected for adenoma tissue. Although no confirmative histopathology was present, patient reached postoperative remission and remained in remission until end-of-study. Scan 3: Female patient in the diagnostic stage of CD with a lesion suspected for a microadenoma on conventional 3T (a) coronal, and (c) sagittal T1 post-contrast MRI, and (d) 3D T1 reconstructed transversal MPRAGE, not visible on (b) coronal T2 post-contrast MRI. (e) [18F]FET-PET-CT image showed focal uptake right paramedian in the sella continuously until right cavernous sinus, concordant with the lesion localization on MRI. Co-registration of (f) coronal, (g) sagittal, and (h) transversal [18F]FET-PET with (i) 3D T1 reconstructed coronal MPRAGE, (j) sagittal MPRAGE, and (k) reconstructed transversal MRPAGE. Confirmative histopathology as well as postoperative remission were achieved after transsphenoidal surgery (TSS). Scan 5: Female patient in the diagnostic stage of CD without a circumscribed lesion visible on conventional 3T (a) coronal T1, (b) coronal T2, (c) sagittal T1, and (d) 3D T1 reconstructed transversal MPRAGE post-contrast MRI. (e) [18F]FET-PET-CT image showed focal uptake left paramedian in the sella. Co-registration of (f) coronal, (g) sagittal, and (h) transversal [18F]FET-PET with (i) 3D T1 reconstructed coronal MPRAGE, (j) sagittal MPRAGE, and (k) reconstructed transversal MRPAGE. In hindsight, the MRI showed a slightly asymmetrical sella as a secondary sign. Histopathology results showed preexistent pituitary tissue with a possible focus of a corticotroph microadenoma, however, this was not sufficient for a confirmative histopathological result, nor did the patient reach postoperative remission. A second TTS also did not result in remission and the patient was treated with bilateral adrenalectomy. Scan 13: Female patient with recurrent CD without a circumscribed lesion visible on conventional 3T (a) coronal T1, (b) coronal T2, and (c) sagittal T1 post-contrast MRI. (d) [18F]FET-PET-CT image showed focal uptake on the left side in the sella. Based on the localization of the primary adenoma this was suspected for an active remnant. Co-registration of (e) coronal, (f) sagittal, and (g) transversal [18F]FET-PET with (h) 3D T1 reconstructed coronal MPRAGE, (i) sagittal MPRAGE, and (j) reconstructed transversal MRPAGE. Despite the confirmative histopathology, the patient did not reach remission. Scan 16: Female patient with recurrent CD with a suspected remnant on the left side of the sella on conventional 1.5T (a) coronal T1 and (b) coronal T2 post-contrast MRI, not visible on (c) sagittal T1 post-contrast MRI. (d) [18F]FET-PET-CT image showed no focal uptake. Co-registration of (e) coronal, (f) sagittal, and (g) transversal [18F]FET-PET with (h) 3D T1 reconstructed coronal MPRAGE, (i) sagittal MPRAGE, and (j) reconstructed transversal MRPAGE. The patient underwent a TSS. During surgery, adenoma suspected tissue was seen on the right side. Although no confirmative histopathology was present, patient reached postoperative remission and remained in remission until end-of-study. Scan 29: Female patient in the stage of recurrent acromegaly with a lesion suspected of a remnant on conventional 3T (a) coronal, (b) coronal T2, and (c) sagittal T1 post-contrast MRI. (d) [18F]FET-PET-CT image showed focal uptake on the right side of the sella, concordant with the MRI location. Co-registration of (e) coronal, (f) sagittal, and (g) transversal [18F]FET-PET with (h) 3D T1 reconstructed coronal MPRAGE, (i) sagittal MPRAGE, and (j) reconstructed transversal MRPAGE. Patient underwent TSS that resulted in confirmative histopathology and postoperative remission. Scan 34: Female patient in the diagnostic stage of prolactinoma with two visible lesions, one of which partly cystic, on conventional 3T (a) coronal T1, and (b) coronal T2 post-contrast MRI. (c) [18F]FET-PET-CT image showed focal uptake on the right side of the sella, concordant with solid component of the cystic adenoma. (d) coronal T1, (e) coronal T2 post-contrast MRI and (f) [18F]FET-PET-CT focused on the right lesion. Patient was treated with TSS which resulted in both confirmative histopathology and postoperative remission
Table 4 [18F]FET-PET results and surgical outcomesOf the 14 surgeries that resulted in confirmative histopathology and/or remission, 12 [18F]FET-PETs were positive (median Likelihood-scale 4.5 [3.3–5.0]). Of the six surgeries that did not result in confirmative histopathology and/or remission, 5 [18F]FET-PETs were positive (median Likelihood-scale 3.0 [2.5–5.0]). Thus, among patients with FPAs with negative or equivocal MRI, the overall sensitivity for localization of functional adenoma was 86% and the PPV 71%, with an overall specificity of 17% and negative predictive value (NPV) of 33%. In CD, the sensitivity was 82% and PPV 69%. The LBR and Likelihood-scale of positive [18F]FET-PETs did not differ between surgeries with and without confirmative histopathology and/or remission (p = 0.171, p = 0.308, respectively).
Diagnostic disease stageThe sensitivity in the diagnostic stage was 86% with a PPV of 86%, a specificity of 50% and NPV of 50%. Within the subgroup of CD, the sensitivity was 83%, PPV was 83% with a specificity of 50% and NPV of 50%.
Persistent disease/recurrenceIn persistent disease and recurrence, the sensitivity was 86% and the PPV 60% with a specificity of 0% and NPV of 0%. Within the subgroup of CD, the sensitivity was 86% and the PPV 60% with a specificity of 0% and NPV of 0%.
Medication prior to and at the time of [18F]FET-PETPituitary-directed agents were not used during, or used more than 6 months prior to, [18F]FET-PET in 26 (70%) scans, continued during 8 (22%) scans, and discontinued within 6 months prior to [18F]FET-PET in 3 (8%) scans. Use of pituitary-directed agents did not alter the proportion of positive [18F]FET-PETs between these groups (p = 0.237), and LBR and Likelihood-scale in positive [18F]FET-PETs did not differ (p = 0.098, p = 0.566, respectively) (Supplemental Table 5).
In CD patients, the only adrenal steroidogenesis inhibitor used was metyrapone, which did not lead to normalization of the 24 h UFC in any of the 3 cases. In acromegaly patients, somatostatin analogues (Octreotide and Lanreotide) with or without a GH receptor antagonist (Pegvisomant), or a dopamine receptor agonist (Cabergoline) were used at time of the [18F]FET-PET in six patients. Despite this use, and biochemical control in three patients (#21, 22, 28), all had positive [18F]FET-PETs (Likelihood-scales 2, 5 and 5). The uptake was assessed with a Likelihood-scale of 5 in all but one due to the concordance with the MRI of a structure interpreted as an intercavernous sinus (#21). Two prolactinoma patients used Cabergoline at time of the [18F]FET-PET, one without achieving biochemical control.
Biochemical activityOverall, the proportion of positive [18F]FET-PETs did not differ between patients with and without confirmed biochemical hypersecretion at the latest assessment before [18F]FET-PET (p = 0.446), neither did the median LBR and Likelihood-scale in positive [18F]FET-PETs (p = 0.248, p = 0.927) (Supplemental Table 5). Time between latest biochemical assessment and [18F]FET-PET did not differ between positive and negative [18F]FET-PETs (median 3.0 months [1.0–5.2] vs. 3.5 [1.0–4.1] (p = 1.000)). No correlations were found between latest 24 h UFC values in CD, IGF-1 levels in acromegaly and PRL levels in prolactinoma and LBR and Likelihood-scale in positive [18F]FET-PETs (Supplemental Table 6).
Biochemical hypersecretion at latest assessment before [18F]FET-PET in CD patients was confirmed in 17 (89%) scans (#19 excluded (median 4.3 months [2.5–8.3] before [18F]FET-PET). In one case of cyclic CD, supported by excessive hair cortisol levels, screening tests before [18F]FET-PET normalized (#15, 1.5 months before [18F]FET-PET). However, [18F]FET-PET revealed focal asymmetric uptake. (Likelihood-scale 4). Last documented IGF-level was increased in 10/14 (71%) scans of acromegaly patients (median 1.5 months [0.0–4.0] before [18F]FET-PET). Last documented prolactin level was increased in all three prolactinoma patients (median 3.0 months (range 1.0–3.0) before [18F]FET-PET). Last documented fT4 level in TSH-oma patient was decreased under thiamazole (1.0 month before [18F]FET-PET).
Follow-upOf the surgically treated patients, 13 patients (65%) reached remission after transsphenoidal surgery and one under medication (Supplemental Table 4). Bilateral adrenalectomy was performed in two patients with a primary diagnosis of CD and in one patient with recurrent CD. Recurrence was seen in one primary and one recurrent CD. A case with suspected recurrent CD and negative [18F]FET-PET (#17) obtained spontaneous biochemical remission during follow-up. It was ultimately concluded that the abnormal screening tests were caused by severe psychosocial stress.
Comments (0)