Patients with IgG4-RD often experience relapse when GC monotherapy is tapered or withdrawn. To reduce both relapse rates and cumulative GC exposure, additional immunosuppressants such as azathioprine are recommended [13].
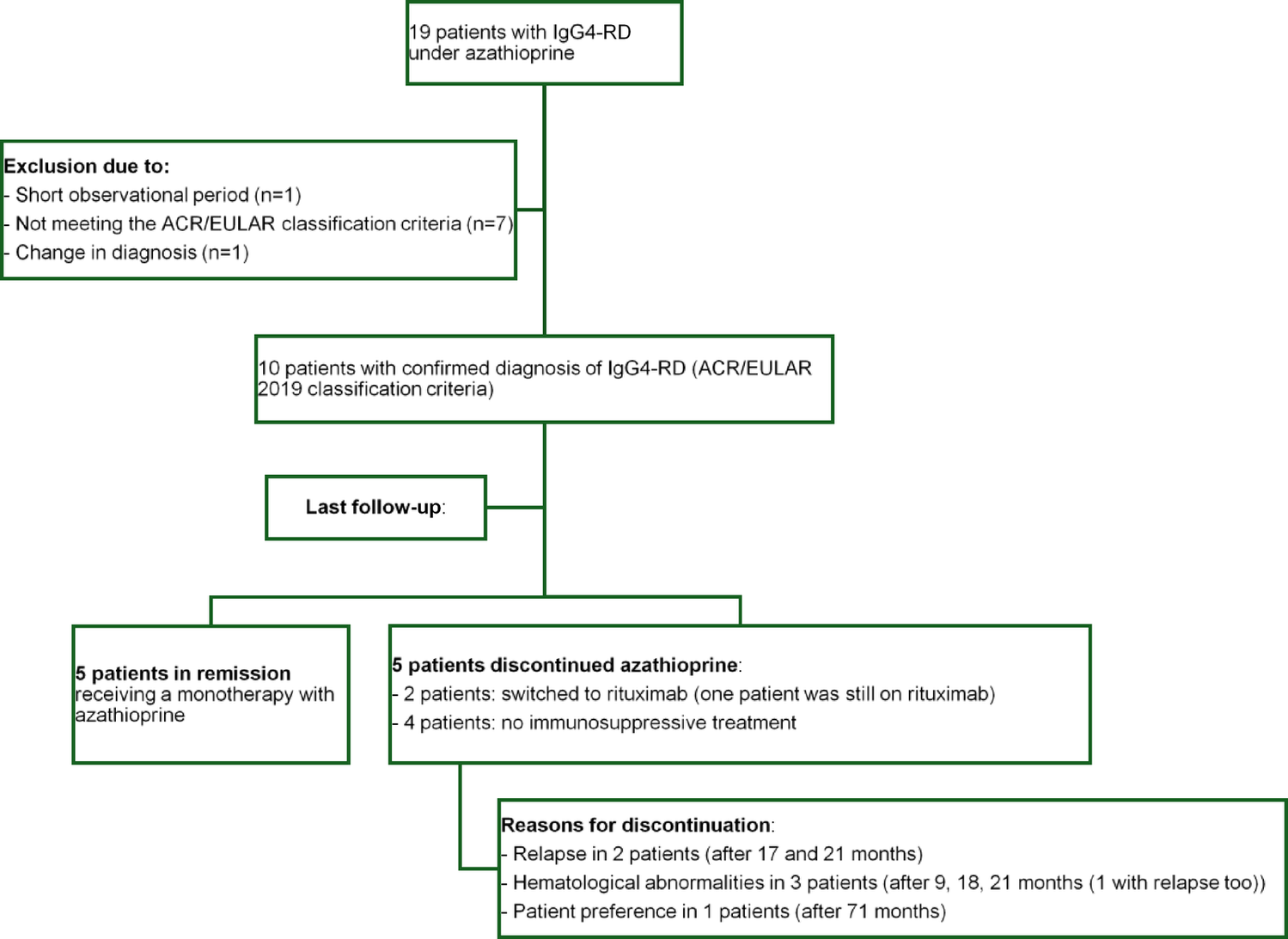
In this study, azathioprine was evaluated as maintenance therapy for IgG4-RD following GC induction. Azathioprine may represent a suitable maintenance option; however, in our small cohort, three patients experienced a total of five relapses during therapy. The safety profile was favorable, with reported adverse events including two infections, four cases of hematologic abnormalities, and one case of elevated liver enzymes. Three patients had to discontinue therapy because of these hematologic abnormalities.
High relapse rates have been reported in IgG4-RD, with both recurrent involvement of previously affected organs and de novo organ manifestations during follow-up. In large cohort studies and a recent meta-analysis by Yang et al. [20] (24 studies, 3,797 patients), cumulative relapse rates were approximately 17% at 12 months, 26% at 24 months, and 33% at 36 months after initial treatment. After GC discontinuation, relapse rates of up to 53% have been reported in patients [13].
Several factors influence relapse risk. The number of organs involved is an independent predictor, with each additional organ increasing the likelihood of relapse [20]. Elevated baseline or persistently high serum IgG4 levels, as well as complement consumption (low C3/C4), have been associated with higher relapse risk. Additional factors include a history of allergy, baseline eosinophilia, and re-elevation of serum IgG4 during follow-up. Withdrawal or tapering of GC is a strong independent predictor of relapse, as confirmed in multiple studies [20,21,22]. In our cohort, patients who relapsed on azathioprine therapy showed persistently elevated IgG4 and total IgG levels, whereas those with normal or normalized IgG4 values remained in stable remission.
In the literature, patients with IgG4-RD who present with hypocomplementemia are described as having a more active clinical phenotype of the disease [23]. In our study complement consumption (C3c, C4) was observed in one relapsing patient. All patients in remission maintained normal complement levels during azathioprine treatment.
Elevated CRP and ESR have also been identified as risk factors for disease relapse [22]. In our cohort elevated CRP at treatment initiation was mainly observed in patients who later relapsed, indicating its potential as a relapse risk marker, whereas ESR declined during therapy regardless of relapse status. Accordingly, our findings suggest that elevated CRP and IgG4 levels may be associated with an increased risk of relapse, even in patients receiving azathioprine therapy.
In 2023, European expert-based consensus statements on the management of IgG4-RD were published [24]. GC are recommended as first-line therapy and should be tapered progressively. Maintenance therapy is advised for patients with high disease activity or relapse risk, using GC-sparing agents, including biologics or conventional DMARDs such as azathioprine, mycophenolate mofetil, leflunomid and methotrexate. Rituximab can be used for both induction and maintenance therapy.
However, no randomized controlled trials specifically evaluating azathioprine in IgG4-RD have been published to date. Current evidence is limited. Small case reports demonstrate efficacy, primarily supporting its use in combination with GC to reduce relapse risk and minimize steroid exposure [25,26,27,28].
Moreover, only a few observational studies with small patient numbers are available, showing inconsistent findings, and in several studies azathioprine was not evaluated as an isolated therapy:
In a Spanish multicenter cohort of 68 patients with IgG4-RD, 13 patients received azathioprine [29]. All achieved partial or complete response (100%; complete response: 45.5 ± 52.2; relapse: 16.7 ± 38.9; treatment failure: 16.7 ± 38.9). In comparison, patients treated with mycophenolate mofetil (n = 6) also demonstrated universal partial/complete response (100%), with a complete response rate of 80.0 ± 44.7, and no relapses or failures. Overall, azathioprine plus GC appeared more likely to achieve partial or complete response compared with surgery alone (OR 3 [0.2–46]).
In a cohort of 53 patients with IgG4-associated cholangitis (IAC), only four patients were treated with azathioprine, of whom one relapsed while on a low-dose of 50 mg/d. In this patient, remission was achieved following an increase in the dose to 2–2.5.5 mg/kg, with no further relapses. All four patients maintained remission on immunomodulatory therapy (median follow-up: 6 months; range, 2–19 months). Based on these findings, the authors suggest an azathioprine dose of 2–2.5.5 mg/kg [30]. However, in our study, weight-adjusted azathioprine doses were lower on average in patients who remained in remission (mean: 1.7 mg/kg/d) compared with those who experienced relapse (mean: 2.08 mg/kg/d).
In a systematic literature review, therapeutic efficacy was demonstrated in 56 of 69 relapses (81%) treated with azathioprine, which was initiated following disease relapse. However, no further analyses specifically evaluating the effectiveness of azathioprine were conducted [31].
In a systematic review of 169 patients with IgG4-related pachymeningitis, azathioprine was administered in 21 cases (12%) [32]. Although relapses were reported during azathioprine treatment, its efficacy was not evaluated independently but rather alongside other immunosuppressants. Notably, azathioprine’s role remains unclear due to the lack of isolated analysis. In contrast, rituximab demonstrated superior efficacy, with a significantly lower rate of refractory disease (3/31; 9.7%) compared to other immunosuppressive agents (11/36; 31%, P = 0.03) in patients with neurological or systemic biopsy-confirmed IgG4-RD.
In contrast to the studies outlined above, a case series of 15 patients with IgG4–related lung disease treated with GC and azathioprine (median treatment duration: 14 months) was evaluated using serial imaging over a median follow-up interval of 12 months. Complete remission was observed only in 2 patients (6.5%), partial remission in 22 (71.0%), and stable disease in 7 (22.6%). Among patients with stable disease as the initial response, two experienced disease progression 10 and 11 months after treatment discontinuation, one achieved partial remission, and one remained stable [16].
In another study including 12 patients treated with azathioprine, only one patient (8%) achieved a complete response [32]. This patient had pancreatic and lymph node involvement, and azathioprine was successfully continued as maintenance therapy following GC induction. Azathioprine was discontinued in 6 of 12 patients (50%) due to toxicity, including hepatic, gastrointestinal, and muscular adverse effects, before treatment efficacy could be adequately assessed. In the remaining five patients, azathioprine failed to sufficiently control disease activity despite treatment durations exceeding three months, leading to discontinuation.
Overall, there is no strong evidence regarding the efficacy of azathioprine across different patterns of organ involvement, whether in single- or multi-organ disease. This study directly provides data on 10 patients with IgG4-RD meeting ACR/EULAR classification criteria, demonstrating an overall favorable response as maintenance therapy and suggesting a potential alternative DMARD strategy. However, the absence of randomized controlled trials and the heterogeneity of outcomes preclude meaningful comparative analyses for azathioprine in IgG4-RD.
Recent randomized controlled and open-label trials have demonstrated encouraging efficacy signals for several alternative GC-sparing agents beyond azathioprine.
In a 12-month, open-label trial, patients with active IgG4-RD were randomized to leflunomide plus GC versus GC monotherapy. Combination therapy was significantly more effective in prolonging the time to relapse compared with monotherapy (HR 0.35, 95% CI 0.13–0.90, P = 0.023) [33].
Another open-label randomized controlled trial included 94 patients with newly diagnosed IgG4-RD, comparing MMF (1–1.5 g/day) plus GC with GC monotherapy. After 12 months, the complete response rate was significantly higher in the MMF + GC group, and the cumulative relapse rate was markedly lower (20.6% vs. 40.0%) [34].
Rituximab, a B-cell depleting therapy, has consistently demonstrated efficacy in IgG4-RD across multiple cohort studies, prospective trials, and meta-analyses [35,36,37]. In a prospective open-label trial, Carruthers et al. [38] treated 30 patients with two doses of rituximab (1000 mg each) without concomitant GC or with successful GC tapering within two months. The primary outcome (IgG4-RD responder index decline ≥ 2 points from baseline, absence of flares before month 6, and no GC use between months 2 and 6) was achieved by 23 patients (77%). At 6 months, 47% were in complete remission, and 40% maintained complete remission at 12 months.
However, another prospective study reported that patients receiving only a single course of rituximab had a relapse rate of 71% after 18 months, compared with no relapses in those maintained on rituximab for 6 months [36]. These findings suggest that while rituximab can induce remission even without GC, maintenance therapy is necessary to prevent disease recurrence.
A phase 3, multicenter, double-blind, randomized, placebo-controlled trial evaluated inebilizumab, a CD19-targeted B-cell-depleting therapy, in adults with active IgG4-RD [14]. A total of 135 patients were randomized, with 68 receiving inebilizumab and 67 receiving placebo. Treatment with inebilizumab significantly reduced the risk of disease flare: Seven patients (10%) in the inebilizumab group experienced at least one flare compared with 40 patients (60%) in the placebo group (HR 0.13, 95% CI 0.06–0.28, P < 0.001). These findings highlight the efficacy of CD19-directed B-cell depletion in reducing flares and promoting sustained remission in IgG4-RD.
Beyond B-cell-directed therapies, several case reports and small series investigating abatacept, belimumab, dupilumab, tocilizumab, and januskinase (JAK) inhibitors have also shown promising results, although robust evidence is still lacking [39,40,41,42,43,44,45,46,47,48].
This study provides valuable real-world data on azathioprine use in patients with IgG4-RD across various organ involvements, all classified by ACR/EULAR criteria 2019. Given the limited existing research on azathioprine as maintenance therapy in IgG4-RD, our findings add information on safety and risk of relapse of azathioprine. Overall, several limitations should be acknowledged. First, the study has a retrospective design. Due to the retrospective design of this study, some data were incomplete or unavailable, which may introduce bias and limit the comprehensiveness of the analysis. Certain clinical or laboratory parameters were not consistently documented. Second, the sample size is small due to the rarity of the disease; furthermore, the strict application of the 2019 ACR/EULAR classification criteria allowed inclusion of only 10 patients from our cohort, although initially 19 patients were considered for inclusion. This reduction may increase the risk of selection bias. Third, the single-center study design limits the generalizability of the findings. Finally, no direct control group was available for comparison with the azathioprine-treated patients, precluding conclusions regarding the effects of different therapeutic strategies.
In this case series, azathioprine may have been less effective in patients with IgG4-RD and renal involvement, however, due to the small number of case, definite conclusion cannot be drawn. Although this observation is preliminary and therefore not generalizable, it is hypothesis-generating and raises the possibility that a stratified approach based on organ involvement and risk profile could be considered in IgG4-RD. Patients could potentially be categorized according to the severity of organ involvement (life-threatening versus mild, non-organ-threatening disease) and therapy could be adapted accordingly. Specifically, in cases of severe organ involvement (e.g., kidney, lung), direct therapy with B-cell-targeted agents may be required to achieve remission, whereas azathioprine might be adequate in patients with mild, non-organ-threatening manifestations.


Comments (0)