There have been no prospective reports investigating long-term local control by PDT and its effect on long-term survival after CRT failure for oesophageal cancer. Usually, salvage surgical treatment is indicated in such cases; however, the morbidity and mortality rates associated with salvage surgery are high. In contrast, PDT is a non-surgical, less invasive treatment that shows a high local complete response (70–90%) for local failure after chemoradiotherapy or radiotherapy for oesophageal cancer. In other words, a complete rather than partial response is the most useful benefit of PDT However, some experts were sceptical that photodynamic therapy may not be effective in terms of long-term prognosis because it is a local treatment. This study aimed to address clinical questions regarding local control (complete response) and long-term outcomes in patients with oesophageal cancer treated with photodynamic therapy as salvage treatment after chemoradiotherapy.
Since PDT is a local treatment, it is unclear how much it contributes to the OS of patients with local failure after CRT or RT for oesophageal cancer. Oesophageal cancer is one of the most intractable cancers and has a poor prognosis. Even patients with T1b oesophageal cancer are at high risk of lymph node metastasis (20–50%). The prognosis of patients who failed CRT or RT with local treatment alone was considered poor.
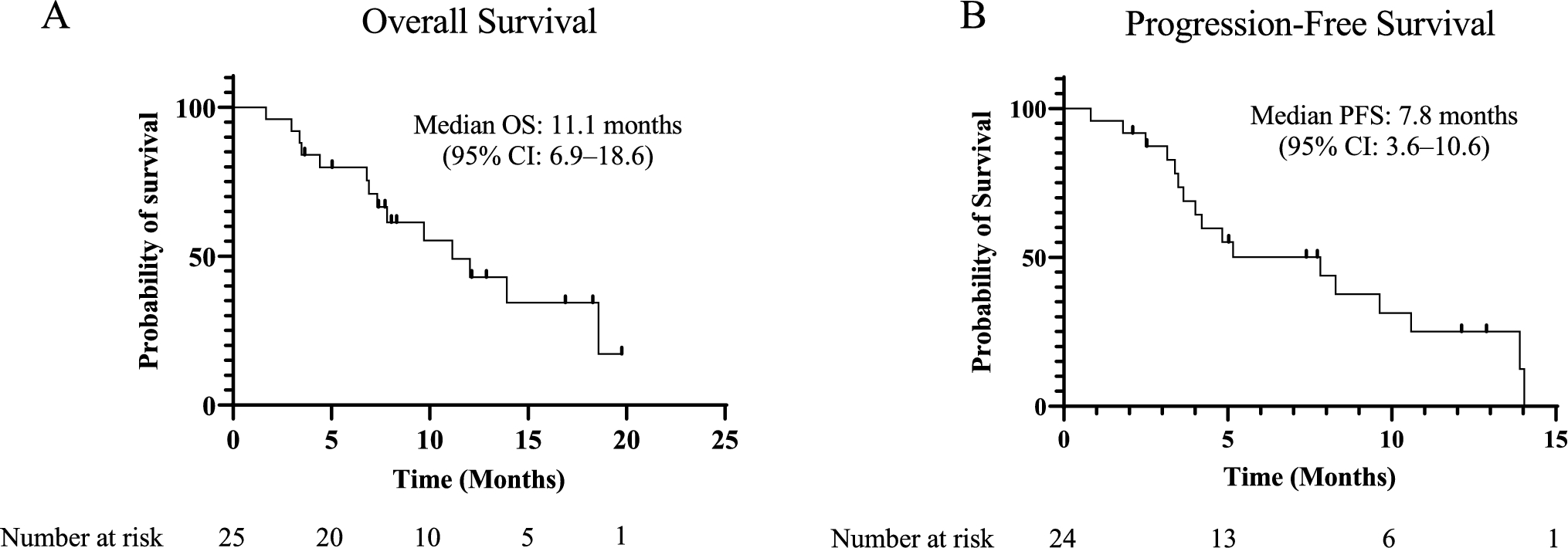
In this prospective 5-year follow-up analysis, talaporfin PDT showed excellent local complete control because only 3 cases of local progression (11.5%) occurred in 26 patients. The 5-year L-TTP rate after talaporfin PDT was 84.9%. This result indicated that talaporfin PDT resulted in effective long-term local complete control. Furthermore, 76.9% (20/26) of the patients did not develop lymph node or distant metastasis, resulting in a median OS of 4.2 years and a 5-year OS rate of 40.6%. Previous research indicated that talaporfin photodynamic therapy (PDT) has a favourable safety profile [20]. To the best of our knowledge, this is the first prospective study to clarify the long-term local complete control rate of salvage talaporfin PDT and its effect on long-term prognosis.
We previously reported that achieving L-CR by salvage PDT was associated with a better prognosis than that of nonCR cases [23]. Minamide et al. also reported that L-CR induced by PDT is associated with longer survival [24]. These reports indicate that local complete control is important to improve patient survival after PDT. However, these reports were made by a single institute and were retrospective. In this multicentre prospective study, we showed not only a high L-CR rate with talaporfin PDT, but also a long CR effect. These results indicate that longer local complete control might be associated with longer OS.
Local recurrence may occur even in patients who can achieve L-CR. In the case of radiotherapy, radical irradiation was performed, and re-irradiation was not possible because of organ toxicity. In contrast, PDT can be re-irradiated. We recently reported that the L-CR rate after repeated PDT was 56.3% and that repeated PDT did not result in any severe adverse events [25]. Yamashita et al. also reported that the L-CR rate after the second PDT session was 40.7% and that there were no severe adverse events [26]. These results indicate that repeated PDT can provide high L-CR even in situations where salvage treatment options are limited, and it is clinically significant as an organ- and function-preserving treatment.
Patients with local, recurrent, or persistent oesophageal cancer after curative definitive CRT are potential candidates for salvage surgery. However, salvage surgery is associated with a high risk of morbidity, including pulmonary complications (29.3%), anastomotic leaks (17.2%), and cardiovascular complications (6.7%) [4]. The 90-day mortality rate was 8.8%. Therefore, minimally invasive and highly curative salvage treatment is required.
In this study, 8 patients (30.8%) had lymph node metastases at baseline, but before PDT, none had lymph node metastasis. Therefore, it is possible that lymph node metastasis was already controlled with CRT or RT. Among the 8 cases, only 1 case showed lymph node metastasis after PDT, but the lymph node metastasis was not present at baseline and was an extraradiation field.
In the T stage before PDT, T1b accounted for 73.1% (19/26) of the cases. Therefore, it is possible that the prognosis was better after PDT. In contrast, a meta-analysis reported that the 5-year OS of salvage surgery after definitive CRT was 24.1% [4]. Sudo et al. reported that among patients with local relapse by definitive CRT, the median OS and 5-year OS rate after salvage surgery were 58.6 months and 45% (95% CI, 26–79%), respectively [27]. Furthermore, Swisher et al. reported that early pathological stage (T1N0, T2 N0) was associated with improved prognosis after salvage surgery [6]. This study showed that the prognosis of talaporfin PDT was comparable to that of salvage surgery, even considering the possibility of controlled lymph node metastasis and the high rate of T1b cases.
Importantly, talaporfin PDT can preserve the oesophagus. No treatment-related adverse events were associated with talaporfin PDT. Therefore, talaporfin PDT may be the ultimate minimally invasive treatment. Considering the loss of organs and high morbidity and mortality rates in salvage surgery, we believe that talaporfin PDT is an important option for salvage treatment. To perform talaporfin PDT, quality control of the procedure is important to achieve L-CR. First, laser irradiation must be precisely applied to the oesophagus, where oesophageal peristalsis is present. Second, if irradiation is judged to be insufficient on the next day’s observation, the endoscopist should perform laser irradiation again to achieve an L-CR. For these reasons, at the time of PMDA approval in Japan, it became a condition of insurance coverage in which a training course was conducted, and the endoscopists were certified.
This study had several limitations. First, this was a single-arm study and was not compared with those of other salvage treatments. Other salvage treatments after failure of definitive CRT for oesophageal cancer include salvage surgery and chemotherapy such as taxane or immune checkpoint inhibitors. However, it might be difficult to conduct a randomised controlled trial with salvage surgery and PDT because their invasiveness is significantly different. In addition, comparative studies with other endoscopic resections (ERs) are also difficult because ER for local failure of T1b and T2 is difficult to perform, and there is no prospective data on ER in a salvage setting. Second, PDT was performed by certified and skilled endoscopists who are experts in PDT treatment. To achieve high CR, laser irradiation must be precisely targeted to the lesion, as previously mentioned. Manuals and training sessions for PDT procedures were implemented to control the PDT quality. This educational and training system is extremely important for widespread clinical use of salvage PDT. Third, this study included only a small number of patients. However, even in a limited number of cases, a high CR ratio represents a significant benefit for patients.
Furthermore, recent in vivo studies in mice have demonstrated that combined treatment with ICI and talaporfin PDT enhances the antitumor effect. Future research should consider the combination treatment with ICI in addition to PDT [28].
In conclusion, talaporfin PDT for local failure after definitive CRT or RT for oesophageal cancer can achieve a long-term local CR and long-term survival. It is an effective and minimally invasive salvage treatment that preserves organs.

Comments (0)