Our study revealed that lung cancer (38%), was the most common primary tumor to exhibit metastatic tumors in the small bowel among Japanese patients followed by colorectal cancer (18%), gastric cancer (9%), and malignant melanoma (6%). Metastatic tumors in the small bowel from renal cancer, malignant melanoma, ovarian cancer, and pancreatic cancer frequently present with gastrointestinal bleeding, whereas those originating from breast, gastric, biliary tract, and ovarian cancers often manifest with symptoms of intestinal obstruction. In contrast, metastatic tumors in the small bowel from lung cancer tend to cause gastrointestinal bleeding and intestinal obstruction with comparable frequency. Predicting the clinical manifestations of metastatic tumors in the small bowel based on the primary tumor type may, therefore, aid the optimization of patient management. In this study, surgery was the only independent factor associated with the prolonged survival of patients with metastatic tumors in the small bowel. To the best of our knowledge, this is the first large-scale study to investigate the clinical characteristics and prognosis of metastatic tumors in the small bowel.
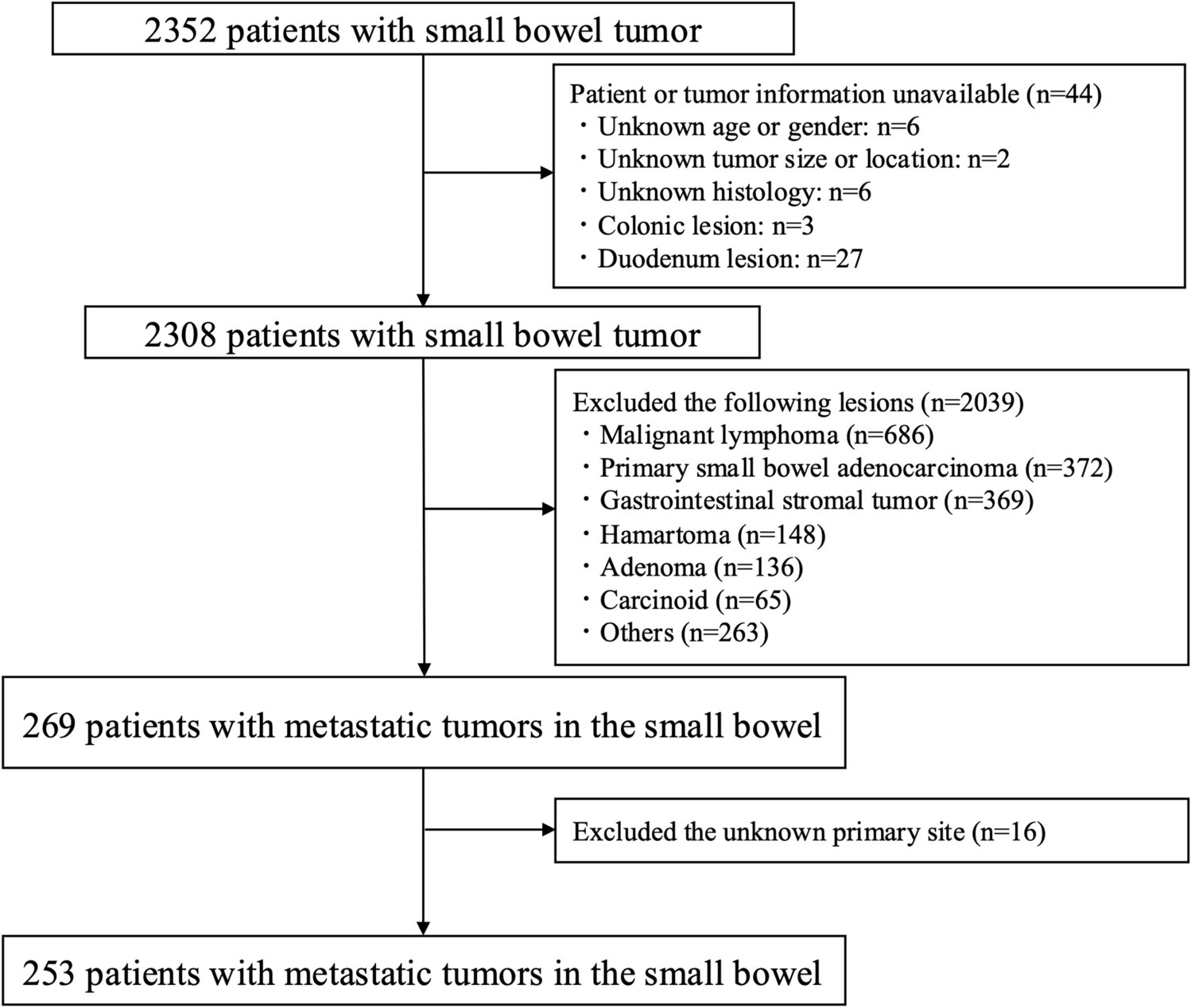
The incidence of small bowel tumors has increased in recent years [2]. Metastatic tumors in the small bowel are generally more prevalent than primary adenocarcinomas in Western countries [18]. In the present study, 253 patients with metastatic tumors in the small bowel were identified, as opposed to 372 patients with primary small bowel adenocarcinomas. This may be attributed to racial differences and the exclusion of patients with direct invasion due to peritoneal dissemination. According to previous reports from Germany, malignant melanoma, breast cancer, and pancreatic cancer are the most common primary tumors to metastasize to the gastrointestinal tract [19]. Gilg et al. [20] reported that among gastrointestinal metastases, the small bowel was the second most common metastatic site after the stomach. They also reported that malignant melanoma, breast cancer, and pancreatic cancer were the leading causes of upper gastrointestinal metastasis, including those in the small bowel [20]. Additionally, in the United States, lung cancer, malignant melanoma, renal cancer, and breast cancer have been reported to metastasize to the small bowel [1, 21,22,23]. A study involving a small cohort of patients from Japan identified lung cancer as the most common primary site, aligning with previous reports [24]. Our findings confirm that lung cancer is the most common primary tumor to exhibit metastatic tumors in the small bowel. However, unlike previous studies, we observed a higher incidence of metastases from gastric and colorectal cancers than from malignant melanoma or renal cancer. Gastric cancer is one of the most prevalent cancers in East Asia, including Japan [25]. Although the incidence of colorectal cancer has declined in the United States in recent years, it remains one of the most common cancers in Japan [26]. By contrast, malignant melanoma is less prevalent in Japan than in Western countries [27]. These differences may be attributed to the variations in cancer incidence across racial and ethnic groups. Indeed, the incidence of each cancer type is known to vary by country and ethnicity worldwide. For example, in Japan, the number of cancer patients in 2024 was approximately 979,000. Among men, the most common cancer was prostate cancer (91,800 patients; 16%), followed by colorectal cancer (85,600; 15%), lung cancer (85,000; 15%), gastric cancer (78,900; 14%), and liver cancer (25,000; 4%). Among women, the most common cancer was breast cancer (91,100 patients; 22%), followed by colorectal cancer (67,600; 16%), gastric cancer (41,200; 10%), lung cancer (36,200; 9%), and uterine cancer (28,300; 7%) [28]. In the United States, the projected number of new cancer patients in 2025 is approximately 2,041,910 [29]. In terms of the estimated number of cancer patients in 2025, the most common cancer among men in the United States is prostate cancer (313,780 patients; 30%), followed by lung cancer (110,680; 11%), colorectal cancer (82,460; 8%), bladder cancer (65,080; 6%), and melanoma (60,550; 6%). Among women, the most common cancer is breast cancer (316,950; 32%), followed by lung cancer (115,970; 12%), colorectal cancer (71,810; 7%), uterine cancer (69,120; 7%), and melanoma (44,410; 4%) [29]. Thus, the epidemiology of cancer varies widely across the world, and this difference in cancer epidemiology may have contributed to the observed findings in the present study. Conversely, because cancer incidence varies across countries, data collected from multiple nations may be subject to inconsistencies. By compiling data exclusively from a single country, such inconsistencies can be avoided, thereby highlighting the rarity of this study.
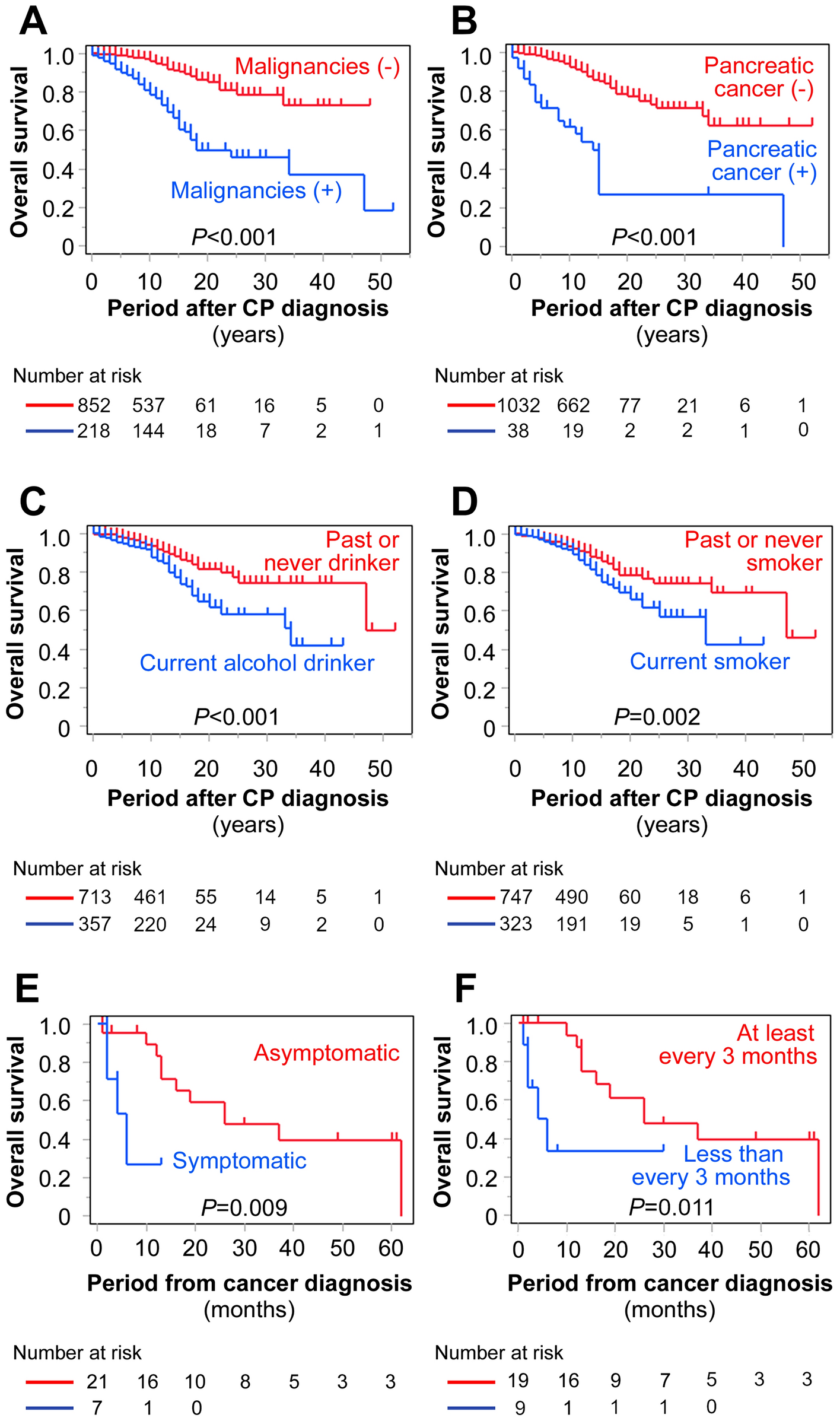
In our study, multivariate analysis revealed that surgery was the only independent factor associated with improved prognosis in patients with metastatic tumors in the small bowel. These tumors can further reduce life expectancy owing to gastrointestinal complications, such as bowel obstruction and gastrointestinal bleeding. Surgery may effectively alleviate these symptoms and improve patient outcomes [30]. Previous reports have also shown that surgical resection of metastases improves OS in patients with metastatic tumors in the small bowel from malignant melanoma [31,32,33]. Additionally, bowel obstruction caused by peritoneal dissemination is often associated with poor OS making surgery unfeasible in certain patients. In such patients, conservative management, including bowel rest, fasting, and intravenous nutrition, is the preferred approach. However, Chouhan et al. [34] reported that in patients of bowel obstruction due to peritoneal dissemination, a combination of transvenous nutrition and chemotherapy is not recommended due to high mortality rates. Therefore, multidisciplinary treatment may not always be the optimal approach, and palliative care should be considered for patients who are not surgical candidates. Endoscopic self-expandable stenting for intestinal obstruction [35] and endoscopic resection for hemorrhagic metastatic lesions [36] may also be considered for symptom management in inoperable patients.
In this study, the presence or absence of chemotherapy had no impact on prognosis. Generally, chemotherapy regimens for patients with advanced cancer and metastases to other organs are comparable to those for primary tumors. Surgery may be required to manage intestinal obstruction or bleeding in patients with small bowel metastasis. However, chemotherapy must be discontinued temporarily if surgery is performed. In our study, 22% of the patients were asymptomatic, and chemotherapy is generally prioritized for such patients. Given the variability in treatment strategies across institutions, establishing standardized criteria for selecting surgery or chemotherapy is essential.
For metastatic tumors in the small bowel, a major concern is the occurrence of gastrointestinal complications, such as bleeding, obstruction, intussusception, and perforation. This study identified gastrointestinal bleeding and intestinal obstruction as the predominant symptoms for the patients with metastatic tumors in the small bowel. Gastrointestinal bleeding was more common in patients with renal cancer (73%) and malignant melanoma (47%) as primary tumors. These cancer types are generally hypervascular [37, 38], suggesting that the characteristics of the primary tumors may have contributed to the signs exhibited by the metastatic lesion. A multicenter retrospective study in France on gastrointestinal metastasis from renal cell carcinoma reported that 70% of the patients presented with anemia and gastrointestinal bleeding [37], which is consistent with our findings. Conversely, patients with breast cancer (60%), gastric cancer (50%), biliary tract cancer (40%), or ovarian cancer (29%) were more likely to have intestinal obstruction [39]. Intestinal obstruction was more frequently observed in patients with primary abdominal tumors, which tended to spread peritoneally. Patients with lung cancer were more prone to gastrointestinal bleeding (25%) and intestinal obstruction (27%). Subjective symptoms are also important factors in identifying the primary site.
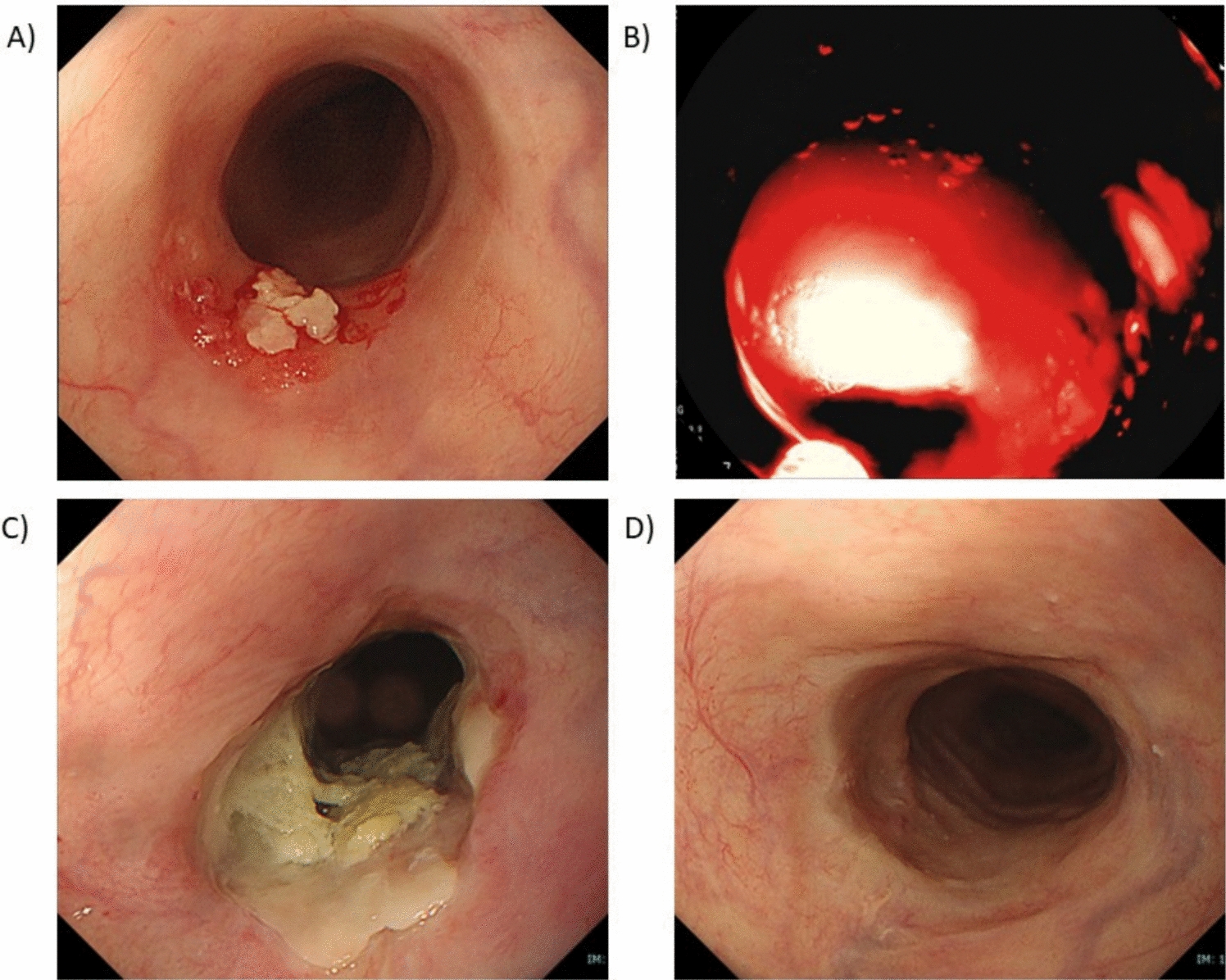
This study has some limitations. First, as a retrospective study, it carries an inherent risk of selection bias, particularly when comparing surgical and non-surgical treatment groups. Patients who underwent surgery may have had better overall health or less aggressive disease, potentially influencing survival outcomes. Although we adjusted for confounding factors, residual bias cannot be completely excluded. Second, the study lacked comprehensive details on the types of surgery performed (e.g., segmental resection and bypass surgery) and their associated postoperative outcomes. The absence of these data limits our ability to assess the true prognostic impact of the different surgical approaches. Further prospective multicenter studies with standardized data collection, including detailed surgical and oncological outcomes, are needed to validate our findings and refine treatment strategies for metastatic tumors in the small bowel. Third, the histology of the primary tumors was not analyzed. For instance, lung cancer is classified into non-small-cell carcinoma and small-cell carcinoma, which require distinct management approaches. Notably, non-small-cell carcinoma frequently metastasizes to the small bowel [11, 40]. Future studies with larger datasets are warranted, to further elucidate the histological types of primary tumors involved, and their associated clinical implications. Fourth, endoscopic evaluation was not performed in all patients. Given the historical context of this long-term retrospective study, the number of patients amenable to endoscopic evaluation using CE or BAE was limited. CE is a minimally invasive modality and is suitable for patients with poor general condition. However, in patients with metastatic small bowel tumors, there is a risk of capsule retention, necessitating careful consideration of its use. Moreover, large lesions may not be fully visualized, which can complicate lesion recognition [41]. Additionally, metastatic gastrointestinal tumors often exhibit submucosal tumor-like morphology [20], potentially leading to false-negative findings with CE [11]. Therefore, the indications for small bowel endoscopy should be carefully evaluated based on the patient’s clinical condition and diagnostic necessity. Fifth, the current study spanned approximately 10 years, raising the possibility of temporal bias in the results. In particular, recent advances in chemotherapy, including the development of novel therapies such as immune checkpoint inhibitors, have markedly improved the prognoses of various cancers. Although the presence or absence of chemotherapy was not associated with improved prognosis in the present analysis, it is possible that chemotherapy may contribute to better outcomes in future studies. Sixth, because the study focused exclusively on malignant tumors of the small bowel, the presence or absence of synchronous metastases to other parts of the gastrointestinal tract could not be analyzed. Gilg et al. [20] reported that among metastatic tumors of the gastrointestinal tract, the stomach was the most frequent site, followed by the small bowel (including the duodenum) and then the large intestine. This suggests that some patients in the present study may have had concurrent metastases in other regions of the gastrointestinal tract. The presence of metastases at other sites can influence therapeutic decision-making, and should be further investigated in future studies. Finally, treatment methods vary across institutions, and no consensus exists on optimal treatment strategies. Further large-scale studies to make up for the lacking information in this study are needed to establish standardized management approaches for metastatic tumors in the small bowel.
In conclusion, the prognosis of patients with metastatic tumors in the small bowel is poor, regardless of the primary cancer. Lung cancer is the most common primary tumor to exhibit metastatic tumors in the small bowel. Surgery was associated with improved OS. Symptoms vary depending on the type of primary tumor. Thus, our findings may guide clinicians in selecting diagnostic strategies and surgical indications based on presenting symptoms and primary tumor type. Small-bowel endoscopies were performed in 33% of the patients as a diagnostic modality. Widespread use of this modality will lead to more frequent accurate diagnoses of such lesions.

Comments (0)