The major findings of this study are as follows. First, patients with CP have a higher SIR for malignancies, with pancreatic cancer being the highest. SIR for pancreatic cancer was particularly high at 29.73 within two years after the diagnosis of CP. Second, age at diagnosis of CP ≥ 65 years and male sex were identified as independent risk factors for pancreatic cancer in a multivariate analysis. Third, SMR was higher in alcohol-related but not in alcohol-unrelated CP. Compared with the previous nationwide multicenter survey conducted in Japan in 2006, the SMR appeared to have decreased [10]. Fourth, among patients with pancreatic cancer, OS was better in those who underwent regular examinations every three months or more frequently compared to those who did not. Lastly, pancreatic cancer was the leading cause of death among malignancies and was identified as the most significant factor associated with overall survival in patients with CP. This study provides updated evidence on the risk of cancer and mortality among patients with CP in Japan.
Previous studies have shown that patients with CP have an increased risk of malignancies. Bang et al. [12], using data from the Danish National Patient Registry, reported a higher risk of malignancies (HR = 1.2), including cancers of the esophagus, small intestine, liver, pancreas, and lung, in patients with CP compared with controls. Han et al. [24] showed that patients with CP had a higher risk of all malignancies (HR = 1.2), esophageal cancer (HR = 3.9), and pancreatic cancer (HR = 3.9) using national claims data in South Korea. Pedrazzoli et al. [25] found a higher incidence of smoking-related tumors, such as lung, esophageal, oral, and pharyngeal cancers, in patients with CP. These results suggest that patients with CP are at an increased risk for malignancies, especially those related to alcohol consumption and smoking. In line with these findings, our study demonstrated that SIR for malignancies was 1.77 in alcohol-related CP but 1.34 in alcohol-unrelated CP. SIRs for alcohol- and smoking-related malignancies such as oral and pharyngeal, esophageal, and lung cancers were higher in alcohol-related CP but not in alcohol-unrelated CP. These findings underscore the importance of cancer surveillance targeting these organs in patients with alcohol-related CP.
Although patients with CP have higher mortality than the general population, the magnitude of this increase, ranging from approximately fivefold [12] to 1.25-fold [20] compared with the general population. These variations can be attributed to several factors, including differences in study periods, populations, etiologies, interventions, study designs, and adjustment variables (including the Charlson comorbidity index and socioeconomic status). In general, patients with alcohol-related CP have higher mortality than those with alcohol-unrelated CP. Miyake et al. [9] reported higher mortality in Japanese patients with alcohol-related CP (by 26.2%) but not in those with alcohol-unrelated CP. The SMR was increased to 2.7 in patients with moderate to severe alcohol consumption, whereas it was not increased in those with none or minimal consumption [26]. These findings are consistent with the more severe natural course observed in alcohol-related CP, which includes the development of diabetes, steatorrhea, pancreatic pseudocysts, pancreatic stones, and biliary stricture, compared to idiopathic cases [27]. Additionally, as mentioned earlier, patients with alcohol-related CP have higher SIR for malignancies compared to those with alcohol-unrelated CP. Continued alcohol consumption and smoking are known to be poor prognostic factors influencing mortality in patients with CP [13, 25, 27]. A Japanese study demonstrated that abstinence from alcohol reduced the risk of pancreatic cancer by five-fold [14]. Since the majority of mortality in CP patients is attributed to extrapancreatic consequences of alcohol and smoking overuse [28], lifestyle modifications, particularly alcohol abstinence and smoking cessation, are essential for improving survival outcomes in patients with alcohol-related CP.
In the previous multicenter study conducted in 2006 on patients with CP registered in 1994, the SMR was elevated in all patients and in males, but not in females [10]. Notably, the SMR decreased from 1.56 to 1.20 in all patients with CP, and from 1.72 to a statistically nonsignificant 1.20 in males. This reduction in SMR, particularly from 2.01 to 1.22 for malignancies, may have contributed substantially to the overall decrease in SMR. However, since the previous study did not report the SIR for malignancies [10], it remains unclear whether the decreased SMR is due to a reduced incidence of malignancies or due to earlier diagnosis. Furthermore, although there is no direct evidence, these improvements might be attributed to recent advances in the management of CP, such as pancreatic enzyme replacement therapy, which is now covered by Japan’s national health insurance. Pancreatic exocrine insufficiency has been identified as an independent risk factor for cardiovascular events and mortality [29], and the absence of pancreatic enzyme replacement therapy has been shown to be an independent predictor of increased postoperative mortality in patients undergoing surgery for CP [30].
CP is a well-established risk factor for pancreatic cancer. A recent systematic review and meta-analysis reported that the risk estimates for pancreatic cancer at 2, 5, and 9 years after CP diagnosis were 16.16, 7.90, and 3.53, respectively [15]. In this study, the SIR for pancreatic cancer was 6.44 across all observation periods and 4.93 after 2 years. The highest risk of pancreatic cancer was observed within the first 2 years (SIR = 29.73), suggesting that some pancreatic cancers are initially missed at the time of CP diagnosis. Munigala et al. [31] suggested that approximately 5% of pancreatic cancer cases are initially misdiagnosed as CP, with a potential diagnostic delay of up to 2 years. Therefore, it is crucial to remain vigilant and not overlook the possibility of pancreatic cancer at or shortly after the CP diagnosis, particularly in cases with ductal dilatation but without calcification. Such cases should be thoroughly investigated to exclude small periampullary tumors that may not be visible on cross-sectional imaging [32].
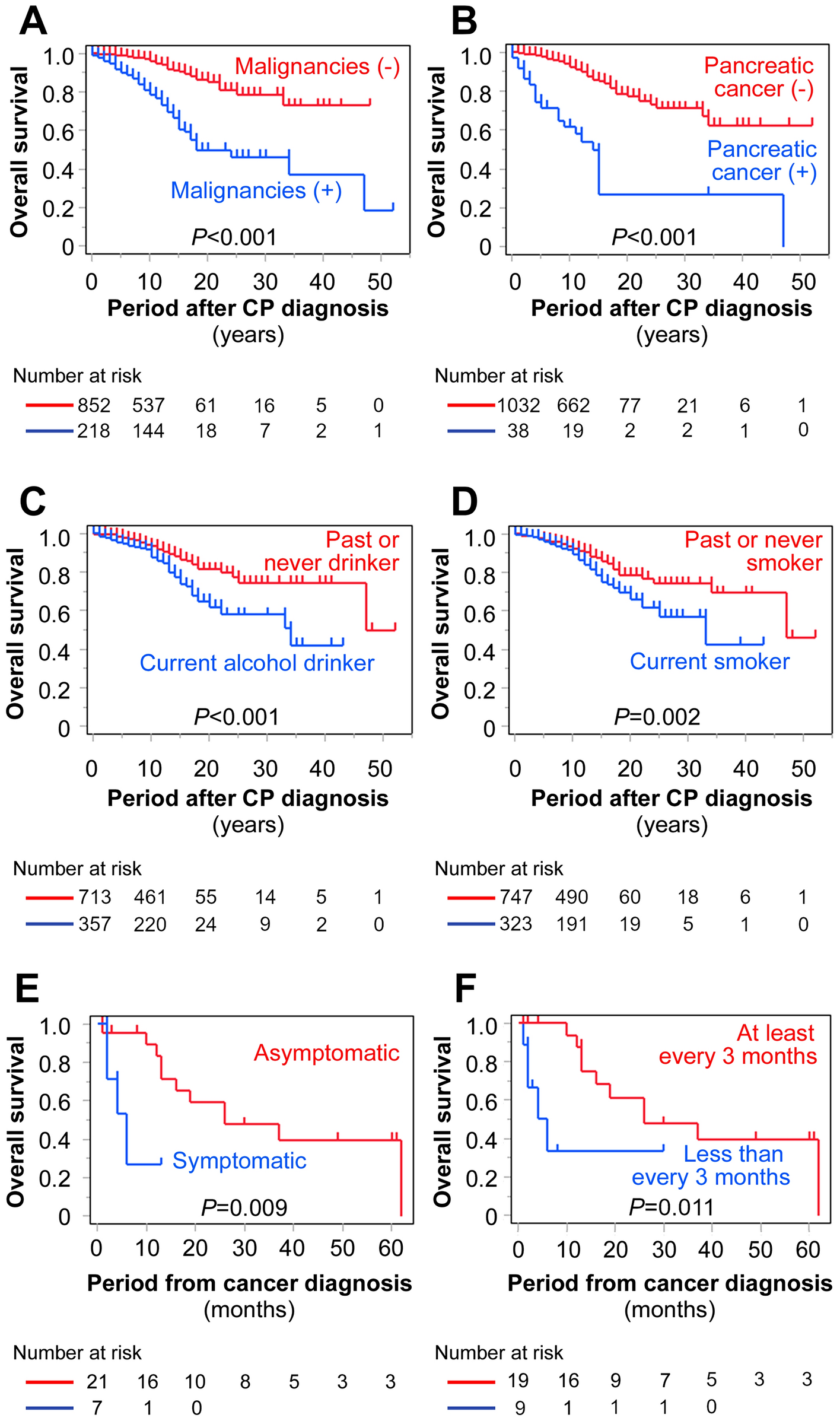
In a recent nationwide population-based cohort study from Denmark, the cumulative incidence of pancreatic cancer after a 2-year latency period was 1% during a mean follow-up period of 16.8 years [33], indicating that the long-term absolute risk is low. In our study, more than half of the pancreatic cancer cases were diagnosed at resectable stages (up to stage IIB) after the diagnosis of CP. The OS of patients with asymptomatic pancreatic cancer was longer than that of those with symptomatic disease, consistent with our previous findings [34]. Notably, among patients diagnosed with pancreatic cancer, those who underwent regular CP follow-up examinations every 3 months or more frequently had better OS than those who did not, underscoring the importance of regular surveillance for early pancreatic cancer detection. To date, a standardized screening strategy for pancreatic cancer in patients with sporadic CP has not been established [35], and no studies have conclusively demonstrated that surveillance improves the prognosis in these patients [36]. Indeed, the standard follow-up intervals varied among the 28 participating institutions: blood tests were performed monthly at one institution, every 2–3 months at two institutions, every 3 months at 16 institutions, every 4 months at one institution, and every 6 months at seven institutions. Imaging studies (most commonly computed tomography and magnetic resonance imaging/magnetic resonance cholangiopancreatography, performed alternately) were conducted every 6 months at 18 institutions and every 12 months at 10 institutions. Identifying an optimal subgroup for surveillance is therefore crucial. Kim et al. [37] identified age over 60 years and serum CA 19–9 levels greater than 100 U/mL as independent risk factors for pancreatic cancer in CP patients. Implementing structured surveillance programs incorporating biomarkers such as CA 19–9 and imaging modalities could potentially reduce mortality and improve outcomes in these patients.
Previous studies have suggested that early surgical intervention for CP may help prevent the development of pancreatic cancer [14, 38]. A multicenter retrospective study in Japan involving 506 patients with CP found that the SIR for pancreatic cancer was 11.8 after excluding cases diagnosed within the first 2 years following CP diagnosis. Over a median follow-up period of more than 5 years, the incidence of pancreatic cancer was lower in patients who underwent surgery (1/147, 0.7%) than in those who did not (18/352, 5.1%). The authors concluded that surgery for CP reduced the risk of pancreatic cancer by approximately tenfold. Similarly, Zheng et al. [38] analyzed 650 patients with surgically managed CP and found that the interval between CP diagnosis and surgery was shorter in patients who did not develop pancreatic cancer, suggesting that early surgical intervention may prevent pancreatic carcinogenesis in patients with CP. The proposed mechanisms underlying this protective effect include the relief of compartment syndrome and inflammation through surgical drainage or resection of fibrotic pancreatic parenchyma, as persistent, uncontrolled inflammation is a well-recognized risk factor for pancreatic carcinogenesis [38, 39]. Given these findings, it is worth investigating whether endoscopic treatments—such as pancreatic duct stenting or stone removal—could similarly reduce the risk of pancreatic cancer by alleviating pancreatic compartment syndrome. In the present study, although endoscopic treatment tended to be associated with a reduced risk of pancreatic cancer in CP patients (P = 0.07), it was not statistically significant.
This study has several limitations. First, it was a retrospective observational study conducted on patients managed in 2011, which may introduce recall bias, and some data were missing. Second, although the SMR was calculated using sex- and age-matched controls, adjustments for comorbidities and socioeconomic status were not possible because relevant data were unavailable. Third, detailed information on laboratory and imaging findings, pancreatic enzyme replacement therapy, and interventions was lacking. Fourth, although our findings suggest that regular examinations may facilitate the early diagnosis of pancreatic cancer, examination protocols were not standardized, and the type and frequency of examinations were left to the discretion of the treating physicians. Lastly, all patients in this study were managed by specialists in pancreatitis care, which may not reflect routine practice in general hospitals across Japan. Consequently, mortality rates might have been underestimated owing to the comprehensive care provided. Despite these limitations, our study provides updated data on cancer risk and mortality among patients with CP in Japan, based on a large cohort of more than 1,000 individuals.

Comments (0)