
Remember me
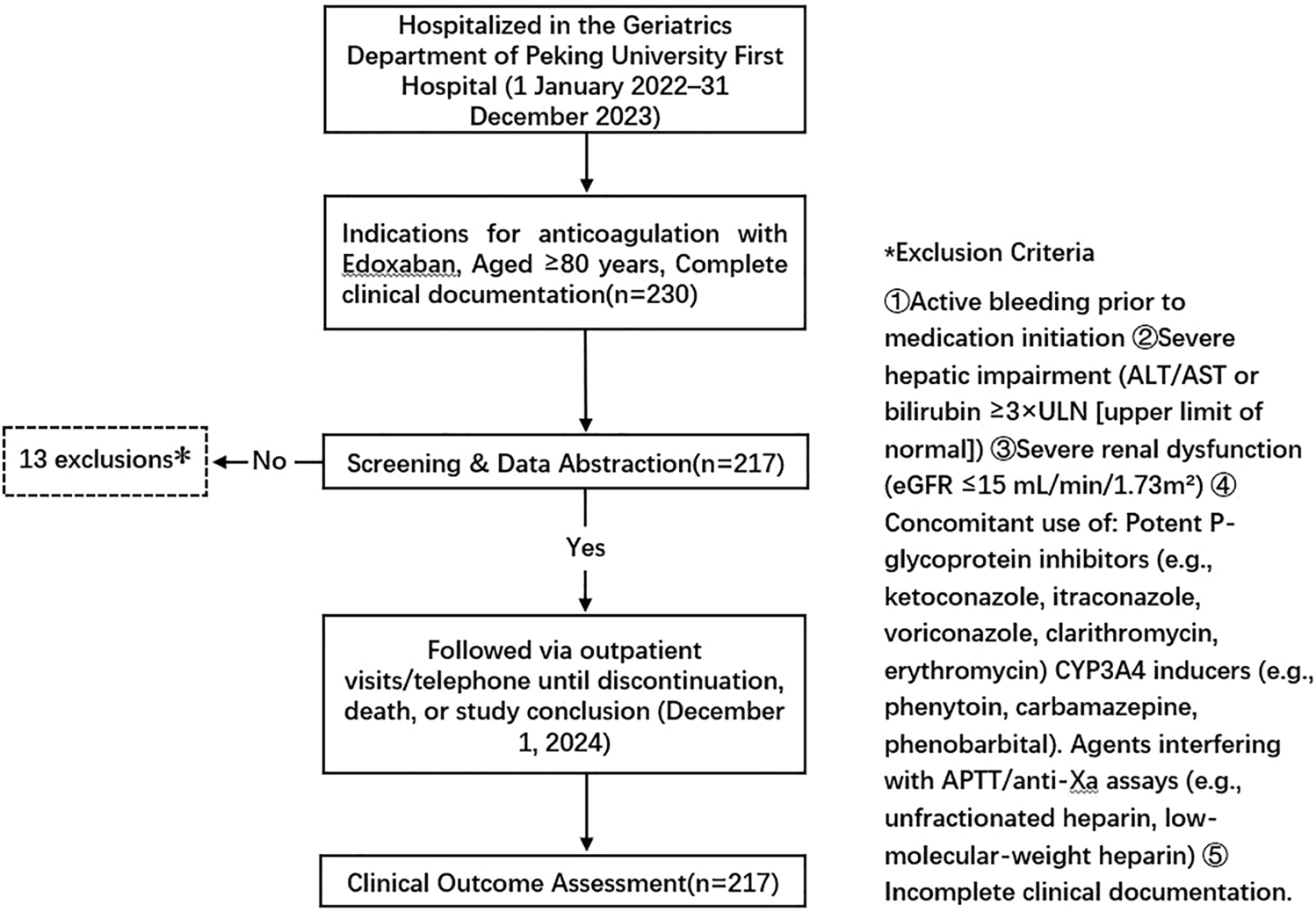

In recent years, China has progressively entered an aging society, with a growing population of advanced older individuals. Since advanced age is a dual risk factor for both thromboembolism and bleeding, anticoagulation therapy in this population poses a clinical dilemma. Current practice among the very old frequently involves the use of nonstandard recommended doses of direct oral anticoagulants (DOACs), where clinicians adjust dosages on the basis of individual patient characteristics. However, the efficacy and safety of such individualized dosing strategies remain controversial [7,8,9,10,11,12].
The current recommended dosage of edoxaban for patients with nonvalvular atrial fibrillation (NVAF) or venous thromboembolism (VTE) is 60 mg/day. However, the dose should be reduced to 30 mg/day in patients with moderate-to-severe renal impairment (creatinine clearance [CrCl] 15–50 mL/min), reduced body weight (≤ 60 kg), or concomitant use of P-glycoprotein inhibitors [1, 2]. However, the mean/median age of participants in previous pivotal clinical trials was 70–73 years [13,14,15,16], which is 5–10 years younger than the actual atrial fibrillation (AF) population, limiting the generalizability of their conclusions to very old patients aged ≥ 80 years [17, 18].
Older patients frequently exhibit multiple comorbidities, high renal insufficiency prevalence, and elevated bleeding risk. For DOAC-treated older patients, clinical practice commonly implements dose adjustments on the basis of clinical characteristics. A Japanese study reported 38.7% reduced-dose rivaroxaban use versus 79.2% for edoxaban in this population [10]. The ETNA-AF-Europe subgroup analysis demonstrated greater reduced-dose edoxaban utilization among frail older individuals [11]. A US community atrial fibrillation survey found 12.5% of older individuals used non-recommended DOAC doses [19]. Chan et al. reported 27% reduced-dose DOAC use [12] versus 51.9% in South Korea [20]. Reduced-dose anticoagulation serves two primary objectives: standard-intensity anticoagulation (stroke prevention in dose-adjusted patients with NVAF) and reduced-intensity anticoagulation (extended VTE treatment). Despite widespread reduced-dose DOAC use, no consensus exists regarding older-specific benefits or personalized dosing protocols (Fig. 2).
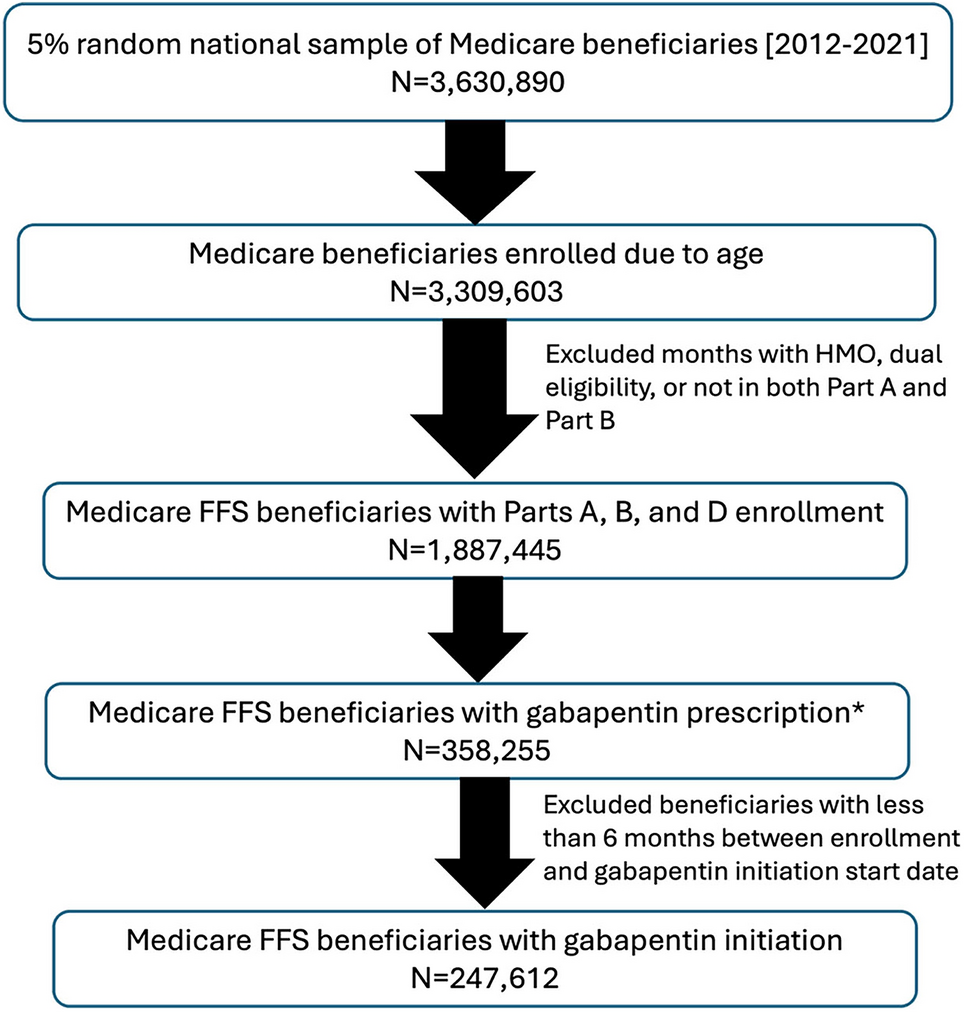
Fig. 2
Hazard functions for mortality in survival analysis between the edoxaban 30-mg-QD and 15-mg-QD groups
Previous studies demonstrate no significant differences in bleeding or thrombotic outcomes between reduced-dose DOACs and standard-dose DOACs/warfarin [21]. A retrospective study observed no significant bleeding or thrombotic risk differences between reduced-dose and standard-dose DOAC groups in octogenarians with atrial fibrillation [22]. Perreault et al. reported reduced bleeding and thrombotic risks with reduced-dose dabigatran versus warfarin (hazard ratio [HR] 0.59) with comparable safety [23]. Fukaya et al. found no significant thrombosis difference between reduced-dose rivaroxaban/edoxaban and standard-dose users with atrial fibrillation [10]. Wei-Chieh et al. identified no significant bleeding/thrombotic risk differences versus warfarin in patients with atrial fibrillation with chronic kidney disease [24]. Suwa et al. studied 348 patients with atrial fibrillation receiving FXa inhibitors; the substandard-dosing subgroup (n = 119) had zero bleeding/thrombotic events during follow-up [25]. A South Korean study showed reduced thrombotic events (HR 0.53) and all-cause mortality (HR 0.57) with reduced-dose rivaroxaban versus warfarin in patients with atrial fibrillation, with comparable bleeding risk (HR 1.10) [20]. Montrasio et al. analyzed 3236 Swiss patients with NVAF and found no significant association between reduced-dose DOACs and major adverse events [26]. Ashraf et al. studied 8125 patients with DOAC-treated atrial fibrillation (n = 1724 off-label dosing), observing no significant differences in bleeding, thrombosis, or mortality between standard-dose and reduced-dose groups [27].
In this study, the edoxaban 15-mg-QD group exhibited significantly older mean age (90.0 versus 85.8, P = 0.001), reduced activities of daily living (ADL) scores (65.5% versus 82.6, P = 0.003), a higher proportion of dependent individuals (75.4% versus 24.6%, P < 0.001), worse renal function, and reduced estimated glomerular filtration rate (eGFR) (58.6 versus 62.6, P = 0.005). These findings suggest clinicians tend to prescribe reduced-dose edoxaban (15 mg QD) for patients with the following characteristics: extreme age (≥ 85 years), functional dependence (ADL ≤ 60), and renal impairment (CrCl ≤ 60 mL/min). This aligns with prior evidence [28], though current guidelines lack standardized dose-reduction criteria, warranting further investigation.
While anti-Xa (AXA) activity reliably reflects the anticoagulant intensity of factor Xa inhibitors, no consensus exists on therapeutic AXA targets for these agents. Clinicians often extrapolate from reduced-molecular-weight heparin (LMWH) standards: prophylaxis in moderate thrombotic risk: 0.10–0.25 IU/mL; prophylaxis in high thrombotic risk: 0.20–0.50 IU/mL: and therapeutic anticoagulation for deep vein thrombosis: 0.5–1.2 IU/mL [29, 30]. Our laboratory uses Hemosil Liquid Anti-Xa detection compliant with internationally certified LMWH standards to ensure global comparability of anticoagulation therapy monitoring results. In our cohort, peak AXA levels reached 0.56 ± 0.25 IU/mL in the 30-mg-QD group and 0.35 ± 0.15 IU/mL in the 15-mg-QD group, both exceeding minimum effective anticoagulation thresholds. This demonstrates that even ultra-reduced-dose edoxaban maintains adequate plasma concentrations in very old patients [18, 31, 32].
The ELDERCARE-AF trial in Japanese octogenarians with AF showed edoxaban 15 mg QD significantly reduced annualized stroke/systemic embolism rates versus placebo (2.3%; HR 0.34, 95% confidence interval [CI] 0.19–0.61, P < 0.001), with comparable major bleeding (3.3%) and all-cause mortality (9.9%) [18]. This study demonstrated significantly reduced all-cause mortality with edoxaban 30 mg QD versus 15 mg QD (HR 0.20, P = 0.044), while exhibiting comparable bleeding and thrombotic event rates. The annualized bleeding rate (2.8%) and major bleeding rate (0.7%) were both lower than those reported in the ELDERCARE-AF trial. Even at reduced doses, edoxaban maintained a favorable safety–efficacy profile in Chinese octogenarians. This may be attributed to strict indication adherence, comprehensive pretreatment assessment (renal function/bleeding/ischemic risks), and individualized anticoagulation regimen development. The mortality advantage in the 30-mg-QD cohort likely reflects baseline disparities; the 15-mg-QD group exhibited more advanced age, higher frailty burden, and worse renal function.
As a retrospective cohort study of high-risk patients ≥ 80 years with multiple comorbidities and medications, our findings reflect real-world anticoagulation practices in China. While limited by sample size and inherent selection bias, these data provide clinically relevant insights for optimizing geriatric anticoagulation strategies.
Comments (0)