2.1 Study Design and Participants
We conducted an analytical cross-sectional study in community-dwelling adults with NCCP. Inclusion criteria were: (1) age ≥ 18 years; (2) fulfillment of IASP diagnostic criteria for chronic pain; and (3) voluntary participation with signed informed consent. Exclusion criteria included: (a) refusal to participate; (b) cognitive impairment that precluded reliable data collection—defined as Global Deterioration Scale (GDS) score ≥ 5 or caregiver-confirmed unreliability; and (c) inability to complete the interview. Institutionalized patients were not excluded per se and were included in the analytical sample (n = 37, 8.1%; Appendix A). However, individuals with advanced cognitive impairment (GDS ≥ 5) were excluded, which may have indirectly reduced the proportion of institutionalized participants.
The sample size was conservatively estimated to ensure both prevalence estimation and adequate statistical power for multivariable analyses. On the basis of prior studies reporting NCCP prevalence between 11 and 50%, we used a 50% estimate, 5% precision, and 95% confidence level, resulting in a required sample of 384. To account for potential data inconsistencies or ineligibility, the target was increased to 455. This sample size also met power requirements for regression analyses. For instance, the least frequently binary outcome with clinical relevance—opioid prescription—had a prevalence of 19%, yielding approximately 86 events, which allows for up to six predictors assuming 15 events per variable. In addition, a priori power analysis using G*Power for linear regression (three predictors: f2 = 0.05, α = 0.05, power = 80%) indicated a required sample size of 160 participants. To ensure analytical robustness, categorical outcomes with fewer than 30 cases (or < 7% prevalence) were excluded from regression models owing to insufficient statistical power and unstable estimates.
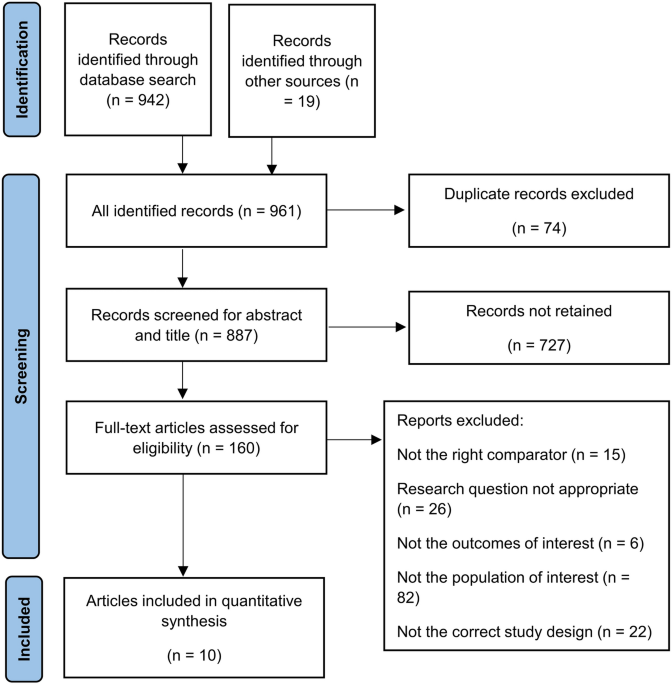
Recruitment was conducted over a 3-month period in two primary care centers in Lugo province (Galicia, Spain). A consecutive sampling strategy was applied: All individuals attending routine primary care consultations during the study period were screened for chronic pain on the basis of IASP criteria. This pragmatic approach ensured systematic inclusion of eligible participants, although it relied on the population attending these clinics rather than a random community-based sample. Of 1646 patients screened, 713 met eligibility criteria, of whom 455 completed the full evaluation and were included in the final sample. Reasons for non-inclusion were logistical constraints (n = 50), refusal to participate (n = 2), and repeated visits by previously included patients (n = 241). Each participant underwent a 20–30 min structured face-to-face interview conducted by trained researchers. Data were collected on 169 variables across multiple domains: demographics (n = 2), chronic conditions (n = 34), pain-related variables (n = 121), self-rated health (n = 1), physical function and disability (n = 4), mental health (n = 5), and social health (n = 1). Additional clinical data were extracted from electronic medical records to complement self-reported information.
The study protocol was approved by the Santiago-Lugo Research Ethics Committee and classified by the Spanish Agency for Medicines and Medical Devices (AEMPS) (LAO-PAR-2018-01).
2.2 Pain Management Variables
Pain management data were grouped into six categories covering the main domains typically evaluated in chronic pain care: (1) initial pain relief strategy, including the type (pharmacological, nonpharmacological, or both) and adherence (5-point Likert scale); (2) prescribed pharmacological treatment, including number, therapeutic class, specific drug(s), administration pattern (intermittent or continuous), and adherence (Likert scale 1–5); (3) self-medication with non-prescribed analgesics, including presence (yes/no), number, drug types, and frequency of intake; (4) nonpharmacological interventions, including number and modality (pain unit invasive techniques, prescribed rehabilitation programs and physiotherapy-based interventions); (5) pain control assessment, including presence of controlled pain (yes/no), degree of control (Likert scale 1–5), satisfaction with control (Likert scale 1–5), and occurrence of breakthrough pain (evaluated only in participants with baseline continuous controlled pain); and (6) healthcare utilization due to pain, including number of visits to primary, hospital, and private care facilities, as well as the number of distinct service types accessed as an indicator of healthcare resource diversity.
2.3 Frailty Index (FI) Construction
To assess global vulnerability and estimate biological age, we constructed a frailty index (FI) on the basis of the deficit accumulation approach, following standard methodology [10, 11, 14]. In contrast to the frailty phenotype, the FI provides a multidimensional and continuous measure of health deficits, making it particularly suitable for our study objectives. Of the 169 variables collected in the study, 42 health-related variables were initially considered for inclusion in the FI; demographic, economic, social, environmental, health behavior, and pain-related variables were excluded [14].
Each variable was recoded on a scale from 0 (no deficit) to 1 (full deficit). Ordinal variables were scaled according to response options (e.g., 0, 0.33, 0.67, and 1 for a four-option variable), and continuous variables were normalized by dividing by their 99th percentile. Two variables were excluded owing to low prevalence (< 1%), while none met the exclusion threshold for saturation (> 80%).
We then examined associations between each variable and age. Variables not significantly correlated with age were excluded (n = 9), with the exception of “rheumatoid arthritis” and “other arthritis,” which were retained on the basis of their well-established age-related prevalence in literature. No variables included in the final index had missing data or high intercorrelation.
The final FI comprised 31 variables across multiple physiological domains (Supplementary Appendix B): chronic conditions (n = 22), self-rated health (n = 1), physical function and disability (n = 3), mental health (n = 4), and social health (n = 1).
FI scores were calculated as the ratio of deficits present to the total number of variables assessed (frailty index = number of deficits present/31). Resulting scores ranged from 0 (no deficits; least frail) to 1 (all deficits present; most frail). For descriptive analyses, we categorized participants into five frailty levels: nonfrail (0–0.1), very mildly frail (0.11–0.2), mildly frail (0.21–0.3), moderately frail (0.31–0.4), and severely frail (≥ 0.41) (ref. 10).
2.4 Statistical Analysis
Descriptive analyses were conducted for all variables. Categorical variables related to pain management were summarized using absolute and relative frequencies with 95% confidence intervals (CI), while continuous variables were described using mean, standard deviation (SD), and 95% CI. For the frailty index, we additionally reported range and 99th percentile to characterize the distribution.
Associations between the frailty index and pain management variables were explored using Pearson or Spearman correlation coefficients, depending on distributional assumptions. Graphical visualizations were constructed to depict trends across frailty strata.
Multivariable linear regression models were fit for continuous outcomes using chronological age, sex, and frailty index as independent variables. We report unstandardized coefficients (B), 95% CIs, and semi-partial correlations to quantify unique contributions. For categorical outcomes, binary logistic regression was applied with the same predictors, reporting odds ratios (OR) and 95% CIs. To ensure the validity of inferences, outcome variables with low prevalence (defined as < 30 cases or < 7%) were excluded from regression models owing to insufficient statistical power and risk of unstable estimates. Multicollinearity between predictors was assessed using variance inflation factors (VIF), and model assumptions (e.g., linearity, homoscedasticity, normality of residuals) were checked via graphical methods and standardized residual diagnostics. Given the exploratory nature of the study and the focus on estimating associations rather than hypothesis testing, no formal correction for multiple comparisons was applied.
All statistical analyses were conducted using IBM® SPSS® Statistics (version 28.0.1.1). No imputation was necessary, as the dataset was complete.



Comments (0)