
Remember me

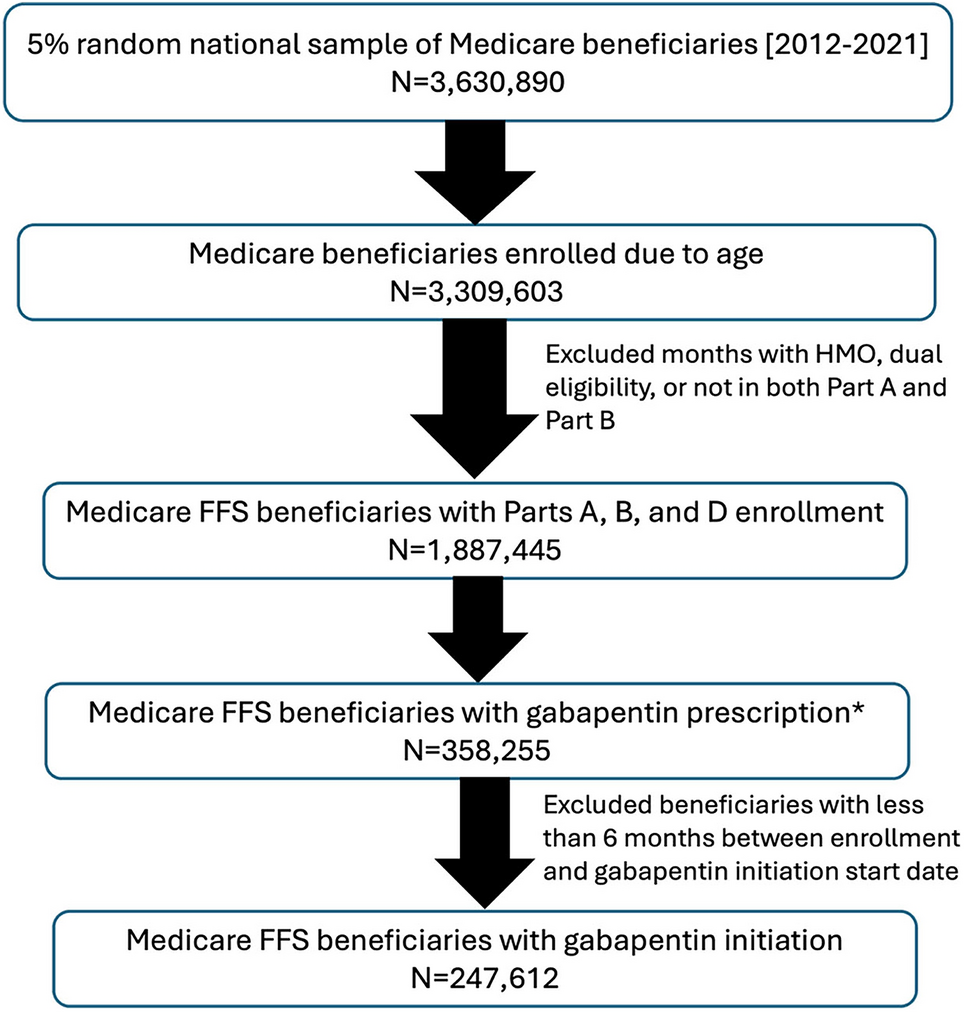
We used a 5% random national sample of Medicare beneficiaries with Part D enrollment at any time from 2012 to 2021. For this study, data from annual Master Beneficiary Summary Files, Part D event files, chronic conditions data warehouse (CCW), outpatient claims, and Medicare Provider Analysis and Review (MedPAR) files were incorporated. Beneficiaries were included if they were enrolled in Medicare Parts A, B, and D owing to age. We excluded the months when beneficiaries had health maintenance organization (HMO) enrollment or were dually eligible for Medicare and Medicaid (Fig. 1). Each beneficiary’s continuous enrollment was determined, allowing for a gap of up to 2 months.
Fig. 1
Sample selection flowchart. *Prescription with extended tablet, solution excluded (N = 35 prescriptions; < 0.01%). Prescription with > 10,000 mg/day excluded (N = 137 prescriptions; < 0.01%). FFS, fee-for service
2.2 Cohort SelectionBeneficiaries with gabapentin prescription were identified if they received at least one gabapentin prescription during their continuous enrollment period. Gabapentin prescriptions were identified using national drug codes (NDC) linked with Medi-span Generic Product Identifiers (GPI), excluding Gralise® Starter. Since the maximum recommended therapeutic dose of gabapentin is 3600 mg/day [27], prescriptions with an average daily dose (dose × quantity/days of supply) exceeding 10,000 mg/day (137 prescriptions) were excluded as likely data entry errors. To mitigate bias from prevalent users, this study included only beneficiaries initiating gabapentin, defined as having at least 6 months of continuous eligibility prior to the first date of gabapentin prescription (i.e., washout period) (Fig. 1). The first date of gabapentin prescription was defined as the index date.
2.3 Prevalence/Incidence of Gabapentin Use by YearThe prevalence of gabapentin use was measured annually from 2013 to 2021. Prevalence was calculated by dividing the number of beneficiaries with at least one gabapentin prescription during the year by the total number of eligible beneficiaries during that specific year. To calculate the incidence rate, the number of new gabapentin users was divided by the total number of eligible beneficiaries in the given year. The year 2012 was excluded owing to the 6-month washout period required to determine initiation.
2.4 Characterizing Gabapentin UseThe average number of days of supply from the first gabapentin prescription were calculated; if multiple prescriptions were present at the index date, the prescription with the longer supply was used. Similarly, the average daily dose from the first prescription was calculated. For beneficiaries with more than one prescription at the index, the average daily doses were summed across all prescriptions. To examine maintained gabapentin dosing, the average daily dose from the second prescription was calculated for beneficiaries with additional prescriptions following the index date.
Demographic information, including age, sex, and race, for gabapentin initiators was obtained from the Master Beneficiary Summary Files. To assess medical history during the 3 months prior to and including the index date—which may provide context for gabapentin prescription, given that data on prescribing reasons were not available—we identified diagnoses for the following conditions: acute pain, back pain, chronic pain, neuropathic pain, epilepsy, postherpetic neuralgia, migraine, depression, alcohol use disorder, and substance use disorder using MedPAR and outpatient files. These conditions were defined using the International Classification of Diseases, Ninth Revision (ICD-9) and ICD-10 codes (Supplementary Table S1) located in the first and second positions of the diagnosis fields.
Similarly, emergency department (ED) utilization was identified if beneficiaries had any ED charge amount recorded in MedPAR files or Revenue Center Codes 0450–0459 or 0981 in outpatient files during 30 days prior to and including the index [28, 29]. Hospitalizations were identified if a record existed in MedPAR during 30 days prior to and including the index, and provider indicator codes were used to classify stays as short-term, long-term, or skilled nursing facility (SNF) stays. Surgical procedures were identified as major therapeutic procedures using ICD-9-Clinical Modification (CM) or ICD-10-Procedure Coding System (PCS) codes from MedPAR files [30, 31] or by applying the surgery flag algorithm using Healthcare Common Procedure Coding System/Current Procedural Terminology (HCPCS/CPT) codes from outpatient files [32] within the same time frame.
Chronic conditions, such as Alzheimer’s disease, diabetes, depression, osteoporosis, hip fracture, osteoarthritis or rheumatoid arthritis, hypertension, atrial fibrillation, congestive heart failure, ischemic heart disease, stroke, and cancer, were examined using CCW files. For the current study, chronic conditions were considered present if their first recorded occurrence date was prior to the index date.
Medication information on CNS depressant use during the 6-month washout period, including opioids, benzodiazepines (BDZ), antidepressants, and antipsychotics, was identified using Part D event files. Antidepressants were further specified by drug class (e.g., serotonin and norepinephrine reupdate inhibitors (SNRIs); selective serotonin reuptake inhibitors (SSRIs); and tricyclic antidepressants (TCA)). Owing to the established risk of concurrent use of opioids and gabapentin, opioid prescriptions at the index date were also examined.
Detailed variable definitions, including specific ICD-9 and ICD-10 and GPI codes used for identification, are provided in Supplementary Table S1. The study design is shown in Fig. 2.
Fig. 2
Depiction of study design and measurement time points
2.5 Continuous Use of GabapentinGabapentin prescription patterns were evaluated using Part D event files. Continuous gabapentin prescriptions were defined as those with a gap of 30 days or fewer between fills. We calculated the number of prescriptions, the mean duration of continuous use (from the index date to the first gap exceeding 30 days), and the average daily dose for 90-day, 180-day, and 365-day follow-up periods. In addition, we determined the proportion of beneficiaries with 100% coverage of gabapentin (allowing for a 30-day gap) over 90 days, 180 days, and 365 days.
2.6 Subgroup AnalysesFor subgroup analyses, gabapentin initiators were categorized on the basis of the duration of continuous gabapentin use: ≤ 90 days, > 90 days and ≤ 180 days, and > 180 days (allowing for a 30-day gap). For each subgroup, we measured demographics, recent medical history, chronic conditions, and healthcare utilization. Furthermore, since the FDA-recommended maximum daily dose of gabapentin is 3600 mg/day, we identified beneficiaries with an initial daily dose exceeding 3600 mg/day (up to 10,000 mg/day), to further describe their demographics, recent medical history, and chronic conditions.
Comments (0)