In this retrospective cohort study, no significant difference was observed in a surrogate marker of efficacy (redosing within 6 h) between low and high doses of antipsychotics in hospitalized older adults. This finding remained after controlling for relevant confounders and evaluating patients with and without hospice or palliative care consultations.
In addition, no major differences in safety outcomes, including LOS, antipsychotic continuation at discharge, or adverse events within 90 days post discharge, were noted between groups. However, higher overall rates of possible antipsychotic-associated adverse events were observed during hospitalization in the high-dose group, though this did not reach statistical significance. Notably, significantly higher rates of in-hospital mortality were noted in the high-dose group (full cohort). While inpatient mortality was significantly higher among patients receiving high doses, the majority of those who died in the full cohort had received a hospice or palliative care consultation, suggesting that their deaths may have been more likely attributable to end-of-life conditions rather than antipsychotic dosage. A significantly higher rate of inpatient pneumonia development was observed in the high-dose group in the non-hospice/palliative care consult subgroup. Antipsychotics have been associated with a myriad of serious adverse events including pneumonia. The increased risk of pneumonia appears to be associated with both first- and second-generation antipsychotic use, which is supported by our investigation, as there was similar use between first- and second-generation antipsychotics among patients who developed inpatient pneumonia (n = 5 haloperidol and n = 7 quetiapine or olanzapine) [22].
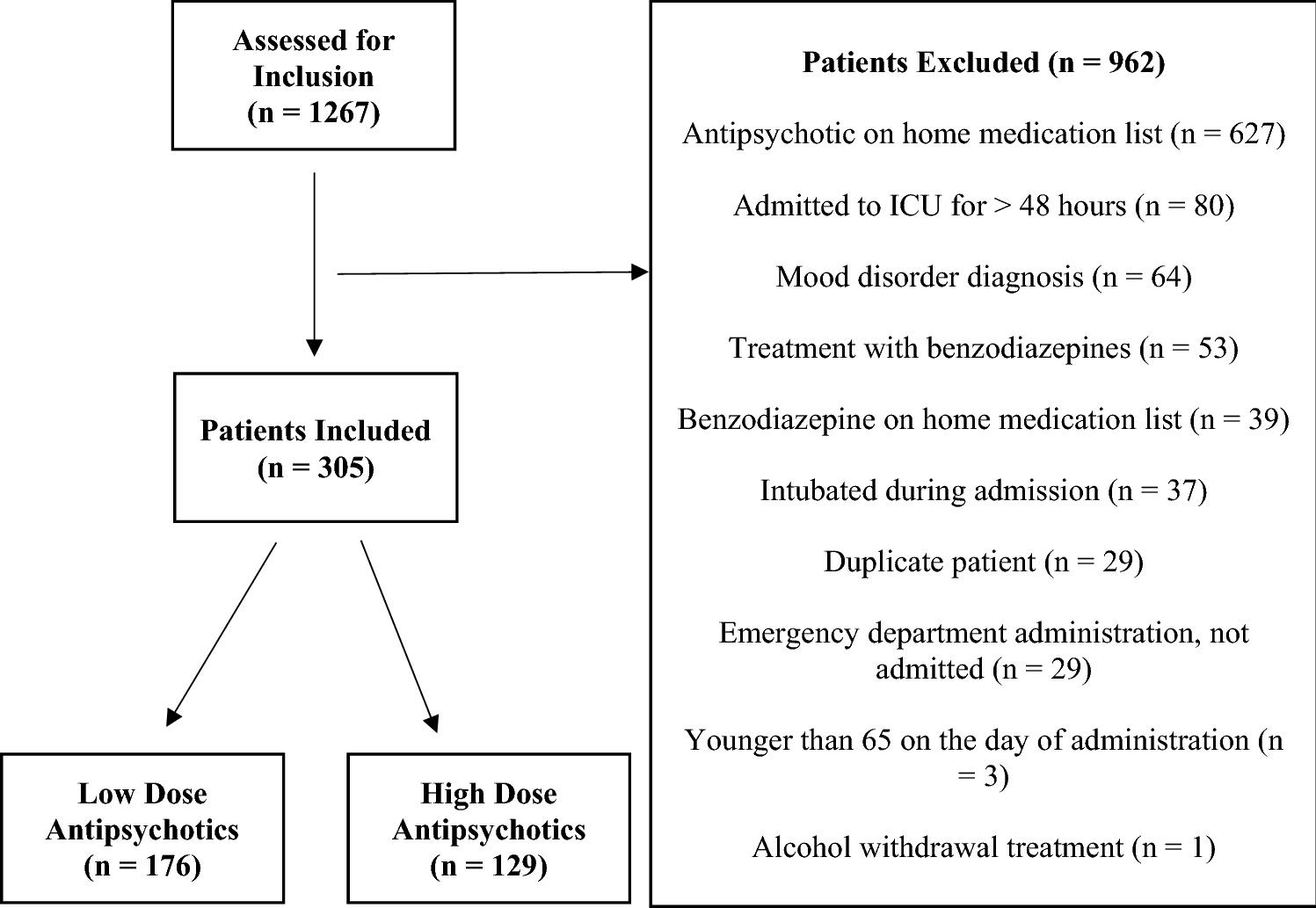
Given the known risks of serious adverse events with antipsychotic use in older adults, clinical guidelines recommend prescribing the lowest effective dose for the shortest duration possible. Despite these recommendations, high doses remain prevalent, as evidenced by the 42.3% of patients in our study receiving high doses (38.1% in the non-hospice/palliative care subgroup). This trend is consistent with prior evaluations of antipsychotic prescribing patterns in hospitalized older adults [23, 24]. Zirker et al. retrospectively analyzed haloperidol dosing in 56 hospitalized older adults with delirium. In this study, 48.2% of patients received high doses (defined as > 1 mg within 24 h). The relative risk (RR) of oversedation was significantly higher in the high-dose group (RR 5.96, confidence interval [CI] 1.44–24.7), and the mean (standard deviation [SD]) duration of agitation was longer, though not statistically significant (3.6 [1.7] versus 6.1 [7.4] days, p > 0.05) [24]. Similarly, Yuksel et al. evaluated 57 older inpatients who received injectable haloperidol. High dose was defined as > 1 mg, which was administered to 33.3% of patients, while low dose was ≤ 0.5 mg. Efficacy, measured by the need for redosing within 4 h, did not differ between groups. However, restraint use was significantly higher in the high-dose group (1 [6.7%] versus 4 [21.1%], p = 0.04) [12]. Notably, these studies had small sample sizes and did not adjust for differences in confounding patient and clinical characteristics in their efficacy analysis [12, 24]. Our evaluation included a significantly larger sample and adjusted for confounding variables but similarly found no difference in efficacy when using higher doses. A more recent retrospective evaluation compared low (≤ 0.5 mg) versus high (> 0.5 mg) injectable haloperidol used in an emergency department in 138 patients ≥ 65 years old. Propensity-score matching was used to match patients in high- and low-dose groups for age, sex, dementia history, schizophrenia, baseline Richmond Agitation–Sedation Scale score, and route of haloperidol injectable administration. There were no significant differences between high- and low-treatment groups with regard to repeat injectable haloperidol dosing within 4 h or the need for physical restraints or safety watch within 4 h. Patients in the high-dose group required an alternative sedative (antipsychotic or benzodiazepine) within 4 h at a higher rate (n = 24 [34.8] versus n = 13 [18.8], p = 0.035) [13]. These findings support the lack of efficacy with use of higher antipsychotic dosage in hospitalized, older adults, as similarly found in our investigation.
While our study assessed olanzapine and quetiapine in addition to haloperidol, a substantial proportion of patients (n = 134, 43.93%) received haloperidol. Furthermore, in a multivariable logistic regression model, haloperidol use was associated with redosing within 6 h of initial administration. This finding aligns with Zirker and Coli’s studies, in which patients receiving higher haloperidol doses had prolonged agitation or required alternative antipsychotic or benzodiazepine administration [13, 24]. Coli et al. hypothesized that patients who received higher doses may have experienced paradoxical (e.g., agitation) reactions to high haloperidol dosage, thus requiring an alternative antipsychotic or benzodiazepine; however, patients in the higher-dose group did receive injectable haloperidol more quickly during their emergency department course, potentially indicating that this group of patients may have been more agitated at baseline [13]. The complex interplay between agitation, delirium, and antipsychotic dosing presents a challenge: While more agitated or delirious patients are more likely to receive antipsychotic therapy, these medications themselves can contribute to altered mental status, potentially exacerbating agitation or delirium. The retrospective nature of previously published studies [12, 13, 24] (and our evaluation) make it difficult to fully ascertain whether higher antipsychotic dosage received was a cause or consequence of increased agitation.
Several limitations must be acknowledged. The retrospective design precludes definitive causal conclusions regarding the effects of antipsychotic dosage. Data collection relied on electronic medical records, which can be inconsistent. Our institution does not routinely document agitation or delirium scores in medically ill patients, preventing the use of a validated agitation or delirium scale to assess the degree of agitation or delirium before or after antipsychotic receipt. This prevented evaluation of agitation/delirium severity in the multivariable models, a notable limitation. Future prospective research should validate this surrogate marker (redosing ≤ 6 h) against clinical scales. We also do not have an institution-specific agitation/delirium protocol for use in older adults on medical floors; treatment decisions were made at the treating physician/medical team’s discretion, which could introduce bias. In addition, selection bias may have been introduced owing to loss of follow-up, as data were obtained from a single health system. Furthermore, we did not capture several confounders that influence delirium and agitation, such as nutritional status, physical activity, sleep quality, or the use of sleep aids such as ramelteon or melatonin. Lastly, a multitude of possible antipsychotic-associated adverse events were assessed to evaluate safety between low- and high-dose groups; however, our work was underpowered to definitively assess the impact of high versus low dosage on adverse events with low incidence rates.
Despite these limitations, our study offers notable contributions to existing literature. Benzodiazepines, known to have paradoxical effects in older adults, were excluded from our study to minimize confounding. Additionally, while previous studies primarily focused on haloperidol, we included newer antipsychotic agents to better reflect contemporary prescribing practices. Importantly, none of the patients in our study were subjected to mechanical restraints, a distinction from prior research. Our findings reinforce the necessity for judicious antipsychotic prescribing in hospitalized older adults, emphasizing the importance of minimizing dose and duration whenever possible. Future research should further explore the relationship between antipsychotic use and adverse outcomes in this vulnerable population.


Comments (0)