
Remember me

To fully appreciate how the gut microbiome may be affected in individuals with obesity, it is important to first clarify some important terms. The human microbiome refers to the diverse ecosystem of microorganisms, including bacteria, fungi, and viruses, as well as their genetic material, that live in and on the human body. Within the human microbiome, the term microbiota refers specifically to the microorganisms living within the microbiome. Finally, the gut microbiome refers specifically to microorganisms and their genetic material that are present in the gut, which are fundamental for optimal physiologic function [53]. It is also critical to appreciate the lack of robust research in humans linking the gut microbiome and obesity, and additional evidence will be needed to determine whether gut microbiome function truly plays a causal role in this setting.
Nevertheless, clinicians increasingly recognize that the gut microbiome likely plays a substantially complex and interrelated role in many conditions and disease states, as evidenced by a wealth of potential relationships described in recent literature [54]. Moreover, the rapid emergence and implementation of artificial intelligence (AI)-assisted microbiome database mining has been leveraged to further elucidate the connections between the makeup of gut microbiota and common diseases [55]. For instance, one review focused on the mechanisms driving an association between the gut microbiome metabolism and the development of hypertension. Contributing factors described included the impact of diet on the gut microbiome, the ability of microbiome metabolites to regulate blood pressure, and the potential for the gut microbiome to impact the relative efficacy of antihypertensive medications [55].
3.1 The gut microbiome and muscle massThe complex interplay between the gut microbiome, obesity and type 2 diabetes also impacts on body composition, especially musculoskeletal health [26]. Furthermore, bone development is greatly impacted by calcium and vitamin D while absorption and activation are impacted by the gut microbiome, leading researchers to suggest a link between the microbiome and bone health from an early age [26]. A direct relationship between the gut microbiome and muscle mass is less well established but is nevertheless a promising avenue as researchers continue to find associations between the gut microbiome and human health [26].
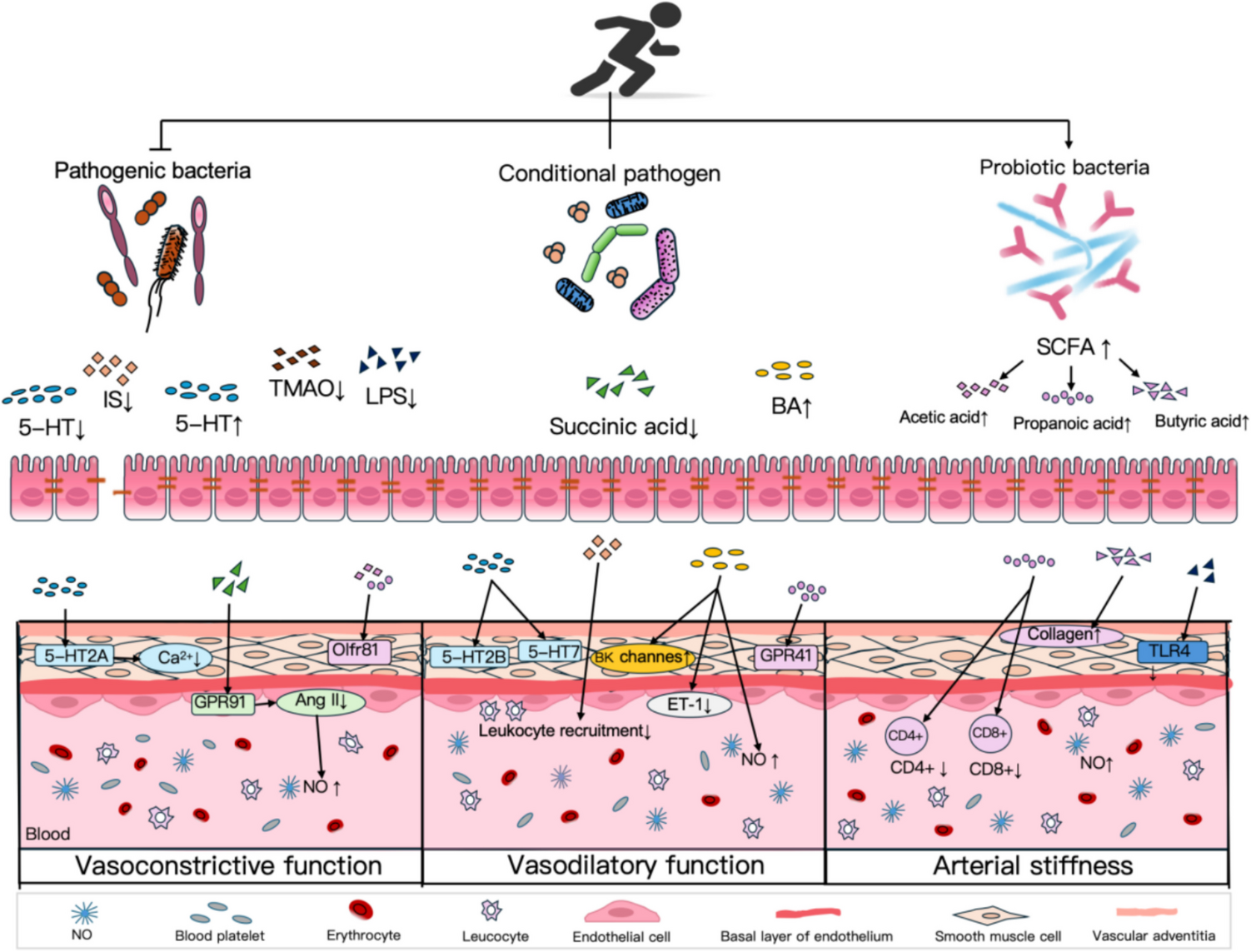
A systematic review of gut microbiome profiles in healthy individuals, including children through adults, reported an association between microbiome composition, lean body mass and muscle mass, especially in athletes [56]. Researchers are especially interested in the gut microbiome as a potential driver of muscle wasting disorders by influencing the degree to which nutrient metabolism by specific microbiota result in conditions such as a pro-anabolic state, inflammation, and insulin sensitivity, among other theories. A visual overview of the potential impact of the gut microbiome on muscle and joints is presented in Fig. 2 [56]. To further support aspects of this theory, a recently completed study investigated the impact of probiotic supplementation on muscle protein synthesis in older adults receiving a plant-based diet. While findings have not been published, the research hypothesis is that probiotic supplementation will positively impact the gut microbiome and enhance the ability to digest plant protein, which in turn will increase amino acid availability that the body uses to synthesize muscle mass [57].
Fig. 2
Influence of the gut microbiome on joints and muscles
Reprinted from: Li R, Boer CG, Oei L, Medina-Gomez C. The Gut Microbiome: a New Frontier in Musculoskeletal Research. Curr Osteoporos Rep. 2021;19(3):347–357. doi:https://doi.org/10.1007/s11914-021-00675-x [56]
3.2 Nutrition and the gut microbiome: implications for patients with obesityNutritional status has a considerable and chronic effect on the gut microbiome, and the status of the gut microbiome likewise influences nutrition. However, research is still needed to determine what nutritional intake strategies best support an optimal gut microbiome, and what constitutes a healthy gut microbiome for individual humans [58,59,60]. Indeed, the presence of some microbiota is associated with beneficial effects in some cases and negative outcomes in others [60].
While continuing research will better characterize the complex associations between nutrition and the gut microbiome, some nutritional strategies have been consistently shown to support gut microbiome function. For instance, adequate dietary intake of insoluble and soluble fiber has been promoted as important to supporting beneficial gut microbiome action, as the microbiota in the gut utilizes these as a source of digestible carbohydrates that results in short-chain fatty acid (SCFA) production. These SCFAs are implicated in modulating inflammation and promoting proper function of the intestinal lining [58, 59]. SCFAs pass into the body’s circulatory system and may likewise cross the blood-brain barrier, suggesting the potential for considerable systemic effects. These may include hormone-induced effects on insulin sensitivity, energy expenditure, and appetite regulation. SCFAs may also impact gene expression that influences host physiology [60]. SCFAs mediate the protein metabolism in skeletal muscle which impacts skeletal function and exercise capacity [61]. While current evidence is confined to studies from animal models, these preliminary findings are promising. However, the complex interactions between nutrition, the gut microbiome, and human health make causative associations challenging. For instance, researchers have reported that excessive circulating SFCAs may have deleterious effects in some cases. In one example, patients with irritable bowel syndrome (IBS) are instructed to adhere to a diet that reduces SCFA production [60].
Microbiota in the gut microbiome is also responsible for the bulk of the digestion of phytochemicals. These naturally occurring chemicals in plant-based foods have demonstrated beneficial impacts on cardiovascular and metabolic health and would otherwise be largely inaccessible to humans without the actions of the microbiota in the gut [58]. In this regard, although excessive protein intake has been associated with metabolites produced by gut microbiota that may be harmful to human health [60], in patients with obesity, dietary protein remains an important strategy to prevent muscle loss, especially during restrictive caloric intake [62]. Amino acids derived from protein may also play a role in serving as markers of metabolic status and influencing other conditions such as the risk of insulin resistance and the development of type 2 diabetes [62].
The ability of the human body to properly produce and absorb micronutrients is also influenced by the gut microbiome. In fact, some microbiota strains produce specific vitamins, vitamin cofactors and micronutrients that can then be metabolized by the human body. Without these organisms, it is possible that humans would be unable to access many micronutrients consumed through dietary intake. These include primarily vitamins K and B12, but vitamin A absorption may also be influenced by microbiota metabolism through the release of vitamin A bound to dietary fiber. Vitamin D has been proposed as a factor in promoting a functional gut microbiome [58].
Current research on nutrition, the gut microbiome, and human physiology suggests a complex interplay among these factors that may nevertheless become a promising avenue to improved nutritional recommendations and treatment strategies for patients with obesity. As many patients with obesity face nutritional challenges through dietary restriction, it is critical to take a nuanced approach in these individuals that reflects the current evidence on gut microbiome health while considering individual intake and other factors that may influence these interactions. Additional research in this promising area is needed to identify nutritional or treatment strategies that support the gut microbiome in patients with obesity.
3.3 Muscle loss prevention and the gut Microbiome in patients with obesityOngoing research may further characterize the complex relationships between nutritional status and gut microbiome function [58, 60], which will determine the best nutritional intervention approaches to mitigate the underlying risk of malnutrition and muscle mass loss in patients with obesity.
While this topic is of considerable research interest to better characterize the interplay between the gut microbiome and body composition, current evidence suggests a complex and beneficial influence of adequate nutrition on both muscle mass and the gut microbiome, which in turn reduces the risk of loss of muscle mass and other inflammation-related conditions in patients with obesity.
3.4 The gut Microbiome and obesityThe composition and function of the gut microbiome not only influences the disease course of obesity and the common comorbidities associated, but it is also directly affected by the presence of obesity and the clinical tools used to treat it, including bariatric procedures and medications that achieve body weight reduction [63,64,65].
Glucagon-like receptor secretion, a target of multiple medications now commonly used to treat obesity and type 2 diabetes, is directly affected by gut microbiome composition [65] and these medications are in turn associated with the promotion of specific gut microbiota [64]. Meanwhile, obesity is independently associated with deviations from the normal metabolism and composition of the gut microbiome, including overall microbiota diversity and the presence of specific bacteria [56, 64]. For instance, a randomized, placebo-controlled trial of inulin-type fructans prebiotic fiber in patients with obesity reported a decrease in a fecal marker of inflammation after three months of treatment [66]. A recent meta-analysis that included 26 randomized controlled trials suggested that probiotics supplementation may be helpful for improving body weight, body adiposity and some cardiovascular risk markers in individuals with overweight and obesity [67].
3.5 Nutrition, obesity, muscle mass and functionalityNutritional status impacts body composition, especially muscle and bone, a fact that guides many of the nutritional recommendations, including those issued by the European Society for Clinical Nutrition and Metabolism (ESPEN) [68,69,70]. Muscle mass is an especially important marker for overall health, and muscle loss is a complex challenge and important therapeutic target in patients with malnutrition [69]. Once underway, loss of muscle mass is difficult to effectively address without substantial nutritional interventions and exercise [69].
Muscle loss is understood as a common consequence of the malnutrition and physical inactivity that often presents in patients with obesity, but the current commonly used terminology– sarcopenic obesity– is confusing and inadequate to effectively define the prevalence of muscle loss in these patients. A joint statement from ESPEN and the European Association for the Study of Obesity (EASO) identified multiple acute disease or nutritional events as suspicion factors that could be used when screening patients for sarcopenic obesity, including recent hospitalizations, recent surgeries with or without complications, recent immobilization, recent decreased food intake (e.g., < 50% for > two weeks), recent body weight loss (including diet-induced voluntary body weight loss and weight cycling syndrome), and long-standing restrictive diets or bariatric procedures [71].
3.6 Health risks associated with muscle loss and functionality (sarcopenia) in patients with obesityThe health risks associated with sarcopenia are considerable. One cohort analysis of older adults included in the population-based Rotterdam Study evaluated participants for low muscle mass and functionality assessed by DEXA and handgrip strength (sarcopenia and sarcopenic obesity according to ESPEN/EASO criteria), and mortality risk over a 10-year follow-up period. After controlling for age, sex, and BMI, those with SO with two altered components of body composition (high fat percentage and/or low appendicular lean mass to body weight ratio) had almost a two- to three-fold increased risk of all-cause mortality. Those with normal handgrip strength and two altered components of body composition (high fat percentage and/or low appendicular lean mass to body weight ratio) were also at an increased risk of all-cause mortality. Importantly, the authors also found that physical activity and protein intake both attenuated this increased mortality risk [72].
Loss of muscle mass in cancer patients with obesity may likewise impact outcomes that have the potential to impact health, longevity and quality of life. In an analysis of 251 patients undergoing surgical resection for colorectal liver metastases, preoperative loss of muscle mass as determined by skeletal mass index measurements (using preoperative computed tomography [CT] scans) was associated with a five-fold increased risk of death (p = 0.01). When evaluating potential predictive factors for disease-free survival, only those with muscle mass loss (p = 0.38) and KRAS positivity (p = 0.041, an established prognostic genetic marker) were significant predictors [73].
Another observational analysis suggests that loss of muscle mass impacts the time required to achieve body weight reduction after bariatric procedures. Patients undergoing laparoscopic sleeve gastrectomy, at a single center, were assessed for body composition by preoperative CT to determine the presence of muscle loss, and outcomes with a primary composite endpoint of body weight reduction and disease-specific quality of life were assessed. Muscle loss was associated with increased time to body weight reduction and lower self-ratings of quality of life. Researchers concluded that preoperative patient assessment for muscle loss may be helpful to tailor rehabilitation guidance [74]. They also stressed that patients with evidence of muscle loss prior to a bariatric procedure should receive preoperative nutritional counseling followed by postoperative rehabilitation, both tailored to the goal of supporting muscle health [74].
Intentional body weight loss in patients with overweight or obesity may also be associated with long-term effects on bone density. The Look AHEAD randomized trial tracked the long-term effects of intentional body weight loss through an intensive lifestyle intervention of reduced caloric intake and increased physical activity versus diabetes support and education in patients with diabetes and overweight or obesity. In one Look AHEAD analysis with a median follow-up of 11.3 years, researchers assessed the association between intentional body weight loss through intensive lifestyle intervention and long-term fracture risk. The analysis found that while patients who underwent intensive lifestyle intervention did not experience an increased risk of incident fractures compared with those who received diabetes support and education, the intensive lifestyle intervention group did have a significant 39% increase in the risk of frailty fractures (HR 1.39; 95% CI, 1.02 to 1.89). Researchers suggested that intentional body weight loss may have a long-term impact on bone density, and that long-term bone preservation should be addressed in patients achieving intentional body weight loss [75].
There is increasing evidence indicating that obesity and sarcopenia both independently contribute to an increased risk of cardiovascular disease. Sarcopenic obesity shares common causes of cardiovascular disease, such as an imbalance between pro-inflammatory adipokines and anti-inflammatory myokines, oxidative stress, and mitochondrial dysfunction. In fact, this metabolic interplay between adipose tissue, muscle, and bone is increasingly recognized in investigations of regulation of body composition. In one study of individuals with metabolic syndrome older than 60 years of age, serum levels of the adipokine adiponectin were inversely associated with skeletal muscle mass [76]. Another study found that adipokines and fat mass index predicted lower bone density in older adults [77]. These factors can lead to insulin resistance, high blood sugar, and high insulin levels, ultimately causing changes in blood vessels, dysfunction in the endothelium, and high blood pressure. On the other hand, chronic cardiovascular diseases, such as heart failure and coronary artery disease, can worsen muscle loss in a continuous cycle [78]. Fat gain and muscle loss are natural consequences of aging, but aging-related sarcopenia is accelerated in individuals with obesity, which in turn increases risks of cardiometabolic disease and early mortality, as shown in Fig. 3 [78].
Fig. 3
Cardiometabolic Consequences of Sarcopenic Obesity
Reprinted from: Mirzai S, Carbone S, Batsis JA, Kritchevsky SB, Kitzman DW, Shapiro MD. Sarcopenic Obesity and Cardiovascular Disease: An Overlooked but High-Risk Syndrome. Curr Obes Rep. 2024;13(3):532–544 [78]
3.7 Addressing nutrition, obesity and muscle loss and gut Microbiome functionA focus on nutrition regarding muscle loss and gut microbiome function is a logical intervention avenue in patients with obesity, as both muscle mass and gut microbiome research continues to describe associations between body composition and the microbiome in health and human disease [56, 63,64,65]. A clinical practice statement from the Obesity Medicine Association (OMA) recognizes microbiome function and its relationship with body weight. The statement highlights common micronutrient deficiencies in patients with obesity undergoing bariatric procedures, including deficits in vitamins A, B1, B9, B12, D, E, and K, as well as deficiencies in minerals including calcium, iron, zinc, and copper [79]. To address these potential deficiencies, the OMA statement notes that high-quality bariatric-specific supplements that include multivitamins, minerals and trace elements are routinely recommended after a procedure, regardless of whether deficiencies are present. The statement also recommends daily protein intake of at least 60 g/day while avoiding excessive caloric intake [79].
Studies are now underway to assess the role of individualized nutritional plans in efforts to optimize the gut microbiome [80,81,82,83] as well as precision nutrition strategies in patients with obesity to specifically impact the gut microbiome [84]. In the meantime, current thinking based on available evidence suggests that patients with obesity, especially those receiving treatment with medications for obesity, should receive nutritional guidance during body weight loss with the goals of maintaining muscle mass, ensuring adequate dietary micronutrient intake, and supporting a healthy, functional gut microbiome.
Comments (0)