
Remember me
This study was preregistered before the analyses were conducted (https://osf.io/ka6n2/). Small adjustments were made during the analysis phase, as described in Supplementary Text 1.
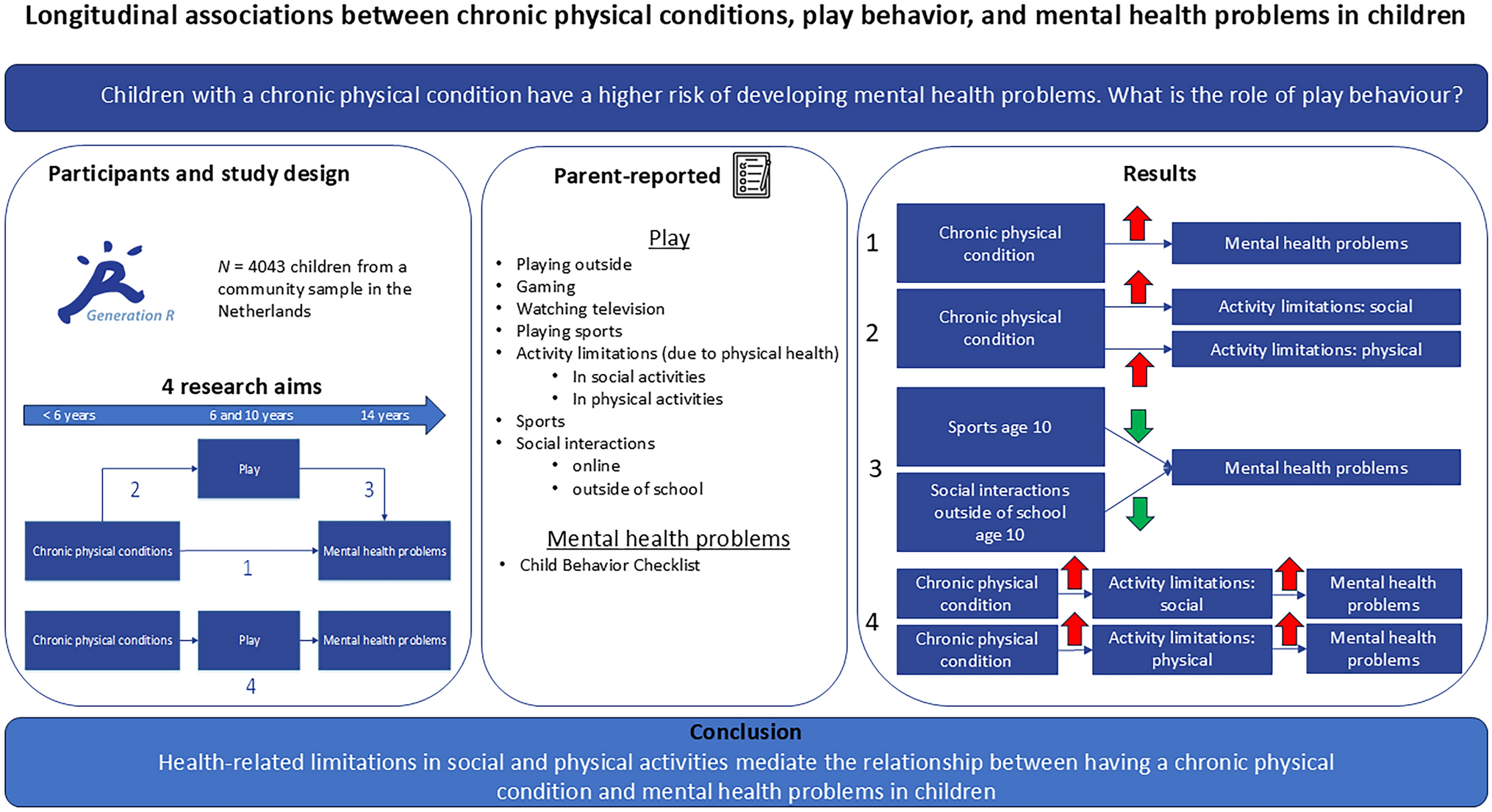
Design and populationFor this study, data from the Generation R Study, a population-based, prospective cohort, were analyzed [19]. The primary aim of this cohort is to investigate the genetic and environmental factors influencing (ab)normal growth, health, and development across childhood into early adulthood. Pregnant women with due dates between April 2002 and January 2006 (and their expected child) were eligible for participation when living in Rotterdam, the Netherlands (participation rate: 61%, n = 9901). The study protocol was approved by the medical ethical committee of the Erasmus MC (University Medical Center Rotterdam, Rotterdam, the Netherlands; MEC 217.595/2002/20), and parents (or legal representatives) of all participants provided written informed consent. Measurement waves were conducted during pregnancy, with follow-ups in childhood and adolescence for those with postnatal consent (n = 7893). Data on outcomes (mental health problems) at the age of 14 years were missing due to withdrawal, loss to follow-up, or nonresponse on this specific questionnaire (n = 5184). Subjects with missing data on chronic physical conditions (n = 666) as well as those with an intellectual disability (n = 8) were excluded from the analyses (Fig. 1).
Fig. 1
Flow chart of study inclusion
MeasuresExposure: chronic physical conditionsIn the original assessment of the prevalence of chronic conditions, van Hal et al. included both physical and mental conditions [1]. For this project, we specifically focused on chronic physical conditions. The following conditions were assessed and identified as chronic physical conditions (mostly before the age of six years): eczema, asthma, morbid obesity, vision impairment, hearing impairment, walking impairment, congenital heart disease, epilepsy, celiac disease, irritable bowel syndrome, and persistent constipation (Supplementary Table 1). In addition, an open-ended question at the age of three years was used to supplement the variable chronic physical condition (“Has your child ever been diagnosed by a doctor as having one or more of the following disorders? Chronic sickness, namely..”). Individual subjects were reviewed and discussed by KEW and NSL (pediatrician).
Data for chronic physical conditions were considered missing (and excluded) when data for fewer than four out of the 11 prespecified conditions were available. The available data were used to define chronic physical conditions as a binary variable (yes/no).
Mediators: play behaviorPlay behavior was parent-reported at the ages of 6 and 10 years. We included measures of the following play behaviors at the age of six years (Supplementary Table 2): playing outside, gaming, watching television (all: average time spent in hours/day), playing sports (no, ≤ 1 hour/week, > 1 hour/week), limited in social activities and physical activities (being restricted in school and social activities due to physical health, being restricted in physical activities due to physical health; yes/no). At the age of 10 years, we defined the following play behaviors: playing outside, gaming, watching television (all: average time spent in hours/day), playing sports (< 1 hour/week, 1–2 hours/week, 2–4 hours/week, > 4 hours/week), social interactions online (chatting and spending time on social network sites; yes/no), and social interactions outside of school (not at all, slightly, quite, extremely).
Outcome: mental health problemsMental health problems of the child were measured at the age of 14 years by the total problem score of the Child Behavior Checklist (CBCL), a component of the Achenbach System of Empirically Based Assessment (ASEBA) [20]. This checklist is a well-validated parent report and consists of 113 items scored on a three-point Likert scale (0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true), where higher scores indicate more emotional and behavioral problems. For boys aged 12–18 years, a score of ≥ 40 is considered borderline problematic, and for girls aged 12–18 years, a score of ≥ 36 is considered borderline problematic. The items can be divided into two broadband scales: internalizing problems and externalizing problems.
CovariatesCovariates were chosen on the basis of their possible relationships with both play behavior and mental health problems. Age and sex were recorded. Ethnicity was categorized as Dutch, other Western, or non-Western, and maternal educational level was categorized as low (no education/primary school/first phase of secondary school), middle (lower or higher vocational training), or high (university). Maternal psychopathology was self-reported by the mother with the Brief Symptom Inventory (BSI) [21]. The global severity index (GSI) was calculated as the sum score of 53 items, with scores for each item ranging from 1 (not at all) to 5 (continually) on a five-point Likert scale. Ethnicity, education, and maternal psychopathology were assessed during pregnancy.
Statistical analysisThe demographic characteristics of participants with a chronic physical condition and participants without a chronic physical condition were compared via independent samples t tests for continuous variables and χ2 tests for categorical variables. A nonresponse analysis was conducted to assess potential selection bias. The demographic characteristics of the sample of responders (n = 4051) were compared to those of participants with missing data on the exposure and outcome variables (n = 5850) via independent samples t tests and χ2 tests. The CBCL total score and continuous play variables were square root transformed variables to meet the normality assumption when included as outcome measures in the analyses. Beta values represent unstandardized effect estimates. Multiple imputation procedures (MICE package, R) were used to address missing values in play behavior and covariates [22]. The variable with the most missing values was social interactions outside of school (23%); therefore, 25 datasets were imputed [23].
The first aim was to investigate the direct associations between having a chronic physical condition, engaging in play behavior, and having mental health problems. We used logistic, ranked-order, and linear regression analyses for binary, ordinal, and continuous outcome variables, respectively. All covariates were included in all the models. In addition, the CBCL total problem score at the age of six years was included as a covariate in the models investigating the direct relationship between play behavior and mental health problems at the age of 14 years to correct for a possible reverse causal effect of mental health problems on play behavior.
Second, we investigated whether certain play behaviors mediated the relationship between having a chronic physical condition and mental health problems. Mediation analyses were performed only if there was a significant relationship between chronic physical condition and mental health problems as well as between having a chronic physical condition and certain play behavior (Puncorrected < 0.05). The proportion of mediation was calculated via regression-based mediation analyses, which were corrected for all covariates and were conducted via the R package CMAverse [24]. We used the default setting for bootstrapping to calculate the 95% confidence intervals (CIs).
Exploratory and sensitivity analyses were conducted for the direct associations. First, if there was a significant relationship between having a chronic physical condition and mental health problems, we conducted a post hoc analysis to determine whether having a chronic physical condition was associated primarily with internalizing problems or externalizing problems. Second, we determined whether participants had a borderline/clinical total score on the CBCL (which corresponded with the ≥ 83rd percentile or a T score ≥ 60). We then repeated the analyses via this binary CBCL outcome measure and applied quasi-Poisson regressions to generate risk ratios (RRs) for improved interpretability. Third, all analyses were repeated with the CBCL measured at the age of 10 years as the outcome to investigate the robustness of our results. Fourth, we repeated the analyses with a broader definition for having a chronic physical condition, complementing the chronic physical condition definition by including the following diagnoses: (food) allergies, lactose intolerance, and a few individual subjects on the basis of the open-ended question about chronic illness asked at the age of three years. Finally, we repeated the analysis investigating the association between having a chronic physical condition and mental health problems after excluding 14 items from the CBCL total score that may directly relate to the chronic physical condition and not necessarily to mental health problems. This included items from the somatic complaints scale and individual items involving overeating, overweight, and bowel movements outside the toilet.
All P values were corrected for the false discovery rate (FDR) via the Benjamini‒Hochberg procedure and considered significant when they were < 0.05. All analyses were conducted via R statistical software packages [25].
Declaration of generative artificial intelligence and artificial intelligence-assisted technologies in the writing processDuring the preparation of this work, the authors used ChatGPT to improve language and readability. After using this tool/service, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Comments (0)