Right Ventricular-Pulmonary Arterial Uncoupling Thresholds in Acute Pulmonary Embolism
Introduction/Purpose
Right ventricle (RV) dysfunction in the setting of acute pulmonary embolism (PE) is associated with worse outcomes. The ratio of tricuspid annular plane systolic excursion (TAPSE) and pulmonary artery systolic pressure (PASP) provides an estimate of right ventricular-arterial (RV-PA) coupling and has been associated with adverse outcomes in patients with pulmonary hypertension. In this study, we examined if RV-PA uncoupling can further risk stratify acute PE.
Methods
This is a single-center, retrospective analysis of patients admitted to a tertiary center with the diagnosis of acute PE. The Kruskal–Wallis Rank Sum, Wilcoxon Rank Sum, and Chi-square tests were used to identify clinical features associated with reduced RV-PA uncoupling at three distinct thresholds, severe (< 0.31), moderate (0.31–0.4) and mild (> 0.4–1.75) derived from prior studies.
Results
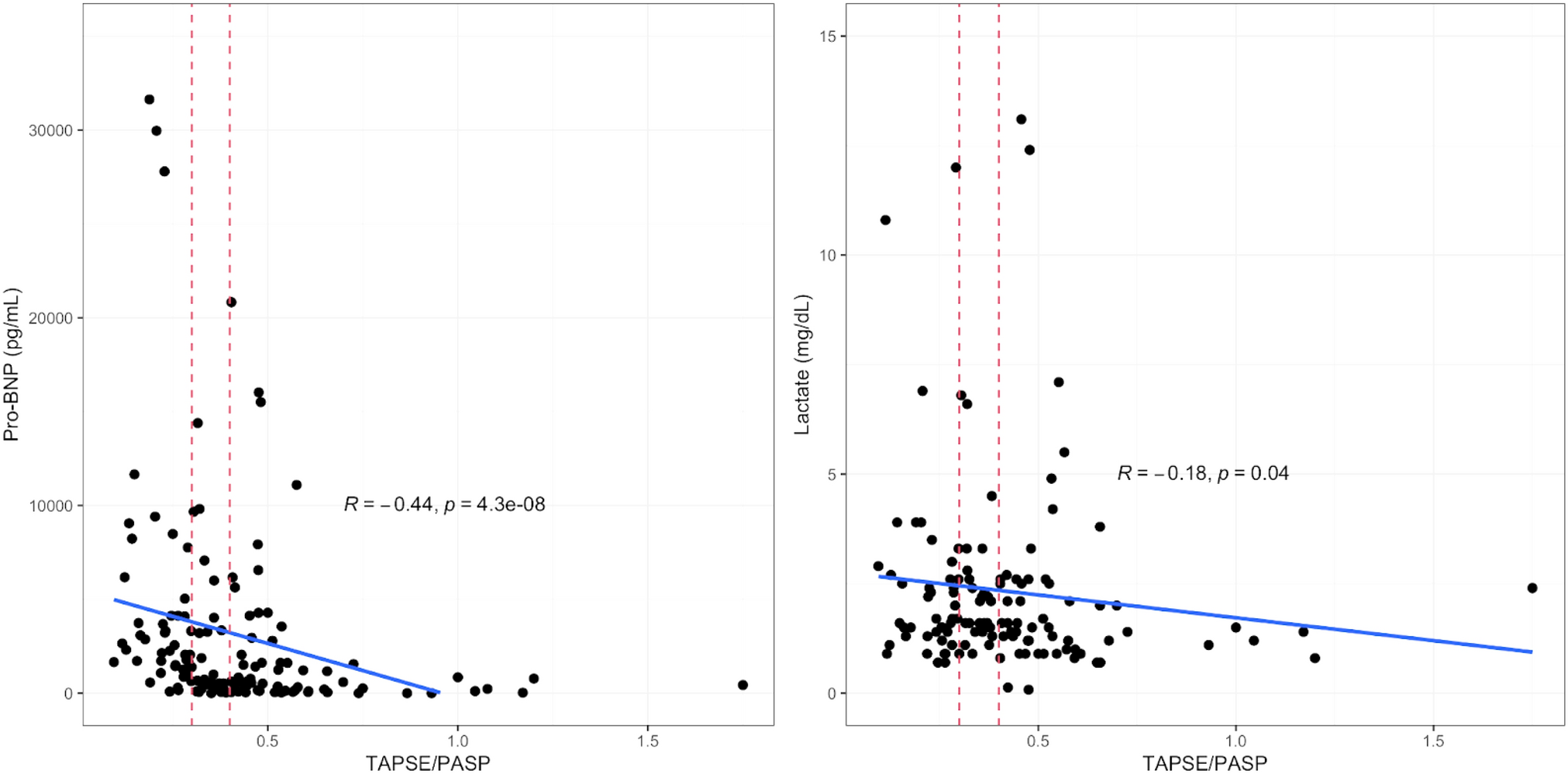
146 patients were included in our analysis. Patients with severely impaired RV-PA uncoupling ratios were more likely to have RV dysfunction by CT defined as CT RV/LV ratio > 0.9 (p < 0.01) and were more likely to need veno-arterial extracorporeal membrane oxygenation (VA-ECMO) compared to those that had moderate or mild impairment (p < 0.01). We also found a correlation between BNP (r = − 0.44, p < 0.01), lactate levels (r = − 0.18 p = 0.04), and the TAPSE/PASP ratio. European Society of Cardiology, sPESI, and BOVA risk stratification scores did not distinguish between patients with mild, moderate, or severe RV-PA uncoupling.
Conclusion
Patients with acute PE who have severely impaired RV-PA uncoupling ratios have more severe disease, characterized by elevated biomarkers and need for VA-ECMO. TAPSE/PASP values can be used to risk stratify and guide treatment of acute PE.

Comments (0)