The FLOW-AF Registry was a multi-country, multicenter, prospective observational study that enrolled patients with NVAF across the MENA region (Egypt, Lebanon, KSA, and UAE). Real-world studies investigating NVAF in the MENA region are scarce, despite the differences in patient profile and management compared with Western countries. To our knowledge, this is one of few studies to prospectively assess characteristics, treatment patterns, clinical outcomes, and HCRU among newly diagnosed patients with NVAF in Egypt.
CVD accounts for approximately 24.58% of total deaths in Egypt, thus ranking Egypt as the 23rd worldwide in terms of CVD-related deaths [28]. A cross-sectional study conducted among 1000 patients with AF in cardiac centers in Egypt showed that HF, hypertension, and CHD were the most prevalent comorbidities [6]. Considering the increasing prevalence of AF/NVAF risk factors in Egypt, generation of local real-world data is critical to support healthcare decision makers to better understand the disease epidemiology and outcomes, and thereby optimize management.
In this study, the mean age of patients was 61.91 years. This is consistent with the findings of a multinational, prospective, registry-based study including 6 Gulf counties, in which the mean age was 57 years [29]. This is also comparable with other research conducted in Egypt (mean age: 59.43 years) and UAE (mean age: 58.6 years) [7, 30]. Results are also replicated in the GARFIELD-AF study which showed that Middle East population was younger than the non-Middle East with median age of 64.0 versus 71.0, respectively [31]. Yet, in contrast, recent Western studies mainly in Europe, Canada, and United States of America (USA) reported a mean age of patients with AF > 70 years [32,33,34], approximately a decade older compared to patients in the Middle East. This younger age profile in the Middle East suggests potential regional-specific factors influencing AF onset, which may require a different clinical approach.
The observed differences between our findings and Western studies may be attributed to several demographic and clinical factors. The higher proportion of male patients in this study may reflect regional healthcare-seeking behaviors or selection biases at participating sites. The lower incidence of thromboembolism and stroke in our cohort is likely related to differences in baseline thromboembolic risk profiles, as evidenced by the lower CHA2DS2-VASc scores compared to Western populations [35]. Additionally, the prevalence of heart failure in this study population was lower than that reported in Western studies, which may have contributed to the observed differences in clinical outcomes and comorbidity burden [36]. These findings underscore the importance of regional and demographic considerations when interpreting data from different populations.
The results showed a high burden of comorbidities among patients with NVAF in Egypt, including hypertension (58.37%), obesity (48.54%), hypercholesterolemia (31.12%), and diabetes (29.88%). These results are in line with findings from the GARFIELD-AF and the Gulf SAFE registry studies, which showed that patients from the Middle East have a high prevalence of comorbidities, such as HF, vascular disease, SE, and diabetes [29, 31]. Additionally, research conducted in KSA and UAE showed that the rate of AF was higher in patients with associated chronic diseases [2, 37]. In contrast, the prevalence of comorbidities among patients with NVAF in Western countries has been reported to be lower compared with the Middle East, e.g., prevalence of diabetes in Canada (20.4%) and Europe (20.6%) is around 10% lower compared with the results of the present Egypt study (29.88%) [38,39,40].
At baseline, most patients had a CHA2DS2-VASc stroke risk score ≥ 2 (67.59%), and the overall mean score was 2.37. This is consistent with findings from other Egypt studies; for example, one study showed that the CHA2DS2-VASc stroke risk score ranged between 2.49 and 3.36 [41], and another revealed 83.5% of patients had a score ≥ 2 [6]. Other studies conducted in the MENA region report similar CHA2DS2-VASc stroke risk score results [2, 31]. In contrast, in the global GLORIA-AF study (N = 15,119 newly diagnosed patients with NVAF), the CHA2DS2-VASc score was higher (median score > 3). Considering older patients are at increased risk of stroke, the higher score in the global study compared to the present study may partly be attributed to the difference in the mean patient age between the 2 studies (72 vs 61.91 years, respectively) [42]. In addition, most of the patients enrolled in the current study did not have a history of stroke (TIA) or congestive HF at baseline (95% and 86%, respectively).
Concerning the HAS-BLED risk score, most patients had a low score (< 3), and the overall mean score was 1.46. This was in line with the Jordan atrial fibrillation (JoFib) prospective, multicenter study (N = 1849 patients with NVAF), which reported a mean (SD) HAS-BLED score of 1.7 (1.1) [42].
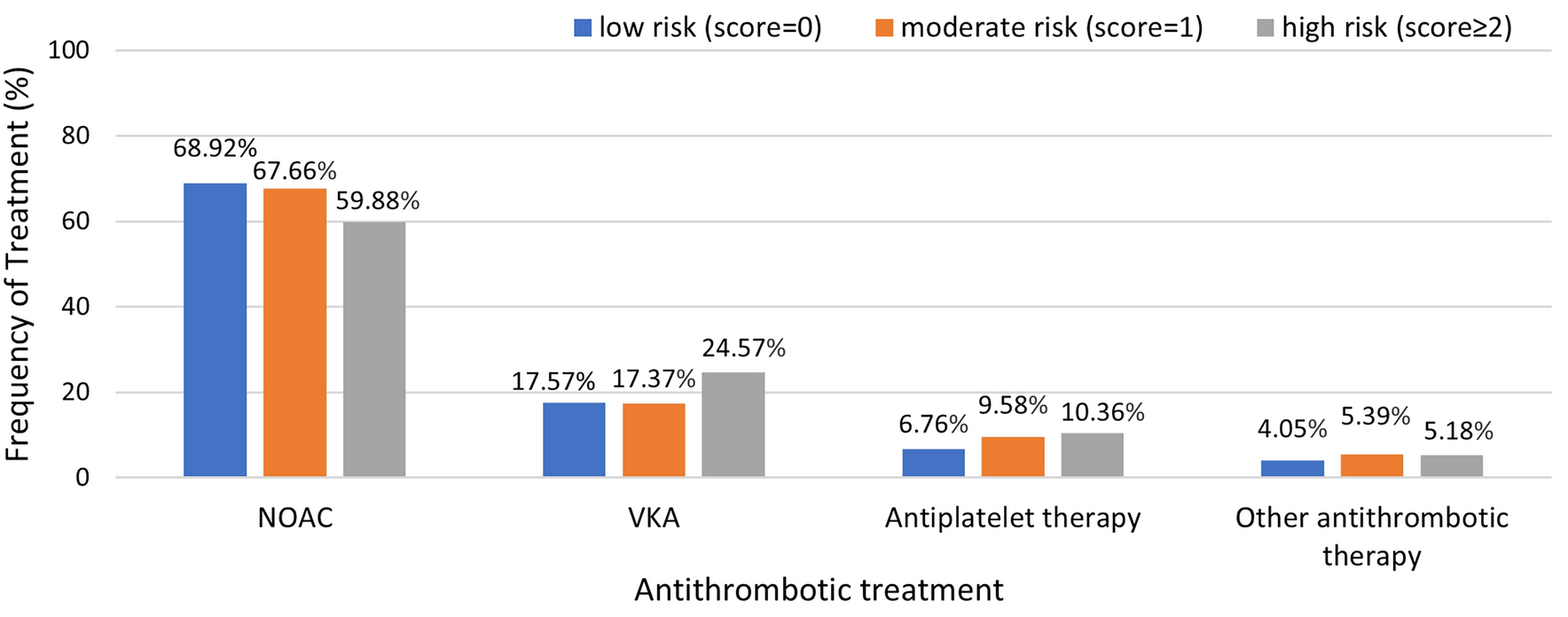
The treatment patterns in this study are consistent with the established global guidelines and recommendations for managing AF [15,16,17,18]. The OACs accounted for > 80% of ATT received by patients, with NOACs contributing 68%, while VKA represented 22.28%. In addition, the antiplatelet therapy constituted 10% of the antithrombotic regimen. These results were similar among patients with CHA2DS2-VASc score ≥ 2 and HAS-BLED risk score ≥ 3, in which NOAC was the most used therapy (59.88% and 48.80%, respectively), followed by VKA (24.57% and 20.48%, respectively). The most frequently used NOACs were rivaroxaban (61.84%) and apixaban (37.11%), indicating they were the preferred NOACs for both initial and subsequent therapy in patients with NVAF. Treatment preferences observed in this study are aligned with findings of other ME, studies including Jordan, UAE, and KSA [2, 44], but contrast with data from other global regions such as North America, Europe, Asia, and Latin America, where VKAs are more commonly used (≥ 32%) [45, 46].
In contrast to the results of this study, the Delta of Egypt Atrial Fibrillation Registry showed high use of VKA (72.6%), with NOAC being used in the minority of cases [7]. This discrepancy may partly be attributed to the type of healthcare setting in each study. While all patients enrolled in the FLOW study were treated in the private health sector and were monitored by PhD-holding cardiologists (which potentially may be associated with better quality of care and elevated use of NOACs), it may be possible that Delta study comprised a more diverse patient pool including those treated in the public sector which has greater access to VKA due to their low procurement costs. Although warfarin has been the gold standard for the prevention of stroke in patients with NVAF for several decades, the FLOW study suggests a modern inclination towards NOACs use, at least within the private healthcare setting. This may be due to the reduced need for frequent monitoring and improved safety profile of NOACs [18, 47, 48].
Moreover, the mean daily dose of rivaroxaban was 18.97 mg with a median of 20 mg and the mean daily dose of apixaban was 8.67 mg with a median dose of 10 mg. These doses are consistent with the specifications outlined in each product label [49].
The 1-year rate of clinical outcomes was low in this study population, with only 4.6% of patients experiencing at least one clinical outcome during the follow-up period. The most frequent clinical outcome was TIA (2.93%), followed by all-cause mortality (0.83%), stroke (0.41%) and bleeding events (0.41%); MI and systemic embolism each occurred at a rate of 0.14%. These rates are lower compared with data from both Middle Eastern and global studies [43, 50, 51]. For example, the Gulf survey of AF (N = 1721 patients with NVAF) reported 1-year rates of 4.2% and 15.3% for stroke/TIA and all-cause mortality, respectively [49]. The JoFib study showed that the 1-year CV mortality was 7.8%, stroke/TIA was 4.5%, and major bleeding events were 2.6% [43]. The low rate of clinical outcomes in our study may partly be related to the characteristics of the patient population (e.g., young age, low mean baseline CHA2DS2-VASc score) and management, including predominant use of NOAC [52,53,54]. Moreover, all participating sites were private hospitals, and participating investigators were all PhD-holding cardiologists; hence, the quality of care received by patients in this study (e.g., including high use of NOACs) may be better compared with the general NVAF patient population in Egypt [55].
Antithrombotic medications accounted for the highest total yearly cost of managing patients with NVAF (per patient per year) (USD 381.9), followed by inpatient admissions (USD 127.9), and surgical/non-surgical procedures (USD 101.8). Laboratory assessments were the most frequently used resource (99.72%) yet accounted for the least total yearly cost (USD 5.4).
Several factors may have contributed to the unusually high annual cost attributed to antithrombotic medications compared to inpatient admissions. Data collection for drug strengths, package sizes, and costs relied on a combination of primary sources and imputation methods. Missing data were addressed by returning to participating hospitals and validating drug names and prices using the official Egyptian Drug Authority (EDA) database. Despite these measures, imputations for certain variables (e.g., package sizes and strengths) may have introduced some uncertainty into the estimates. Furthermore, the COVID-19 pandemic may have reduced hospital admissions and clinic visits, potentially underestimating inpatient costs during the study period. Despite these limitations, the analysis provides critical insights into the economic burden of NVAF management in Egypt and highlights areas for future investigation, such as incorporating sensitivity analyses and extending the dataset to include longer follow-up periods.
A greater total annual cost of ATT than inpatient admissions is an unusual finding of this study, which may be explained by several factors. First, there were limited data on drug strengths and package sizes in the FLOW registry, which necessitated imputations, potentially impacting the medication costs. Second, the COVID-19 pandemic may have influenced the frequency of hospitalizations and clinic visits during the time of this study, thereby resulting in an underestimation of costs related to inpatient admissions. Third, it is possible that errors in recording resource costs in the costing questionnaire may have occurred at the site level (e.g., for insured patients, only costs incurred at the individual patient level may have been recorded). The HCRU and cost data in this study should be interpreted taking into account these caveats. Despite these limitations, this study is one of the first to shed light on HCRU/associated costs among patients with NVAF in Egypt and paves the way for further research to expand on these results.
Limitations
This study has several limitations inherent to its observational design, including potential bias and confounding. The exclusive enrollment of patients from private healthcare facilities limits the generalizability of the findings to the broader Egyptian population, particularly those treated in the public sector, where access to advanced resources, such as NOACs, and specialized care may differ significantly. The inclusion of patients managed by PhD-holding cardiologists in private hospitals may have influenced the observed outcomes, reflecting optimal care scenarios rather than the full spectrum of care available in Egypt. The COVID-19 pandemic may have further impacted the study results by disrupting patient recruitment and follow-up due to movement restrictions and healthcare resource reallocation. However, healthcare access in Egypt remained largely uninterrupted, with primary PCI drugs and essential medications being adequately supplied, which minimized disruptions in NVAF care. Nonetheless, the pandemic’s indirect effects on healthcare utilization, such as reduced hospital visits due to precautionary measures, may have influenced the observed outcomes.
Another limitation of this study is the lack of detailed data on heart failure (HF) phenotypes. The absence of this information prevents a more nuanced analysis of the relationship between NVAF and different HF subtypes, such as HF with preserved ejection fraction (HFpEF) or reduced ejection fraction (HFrEF). This limitation may have influenced the interpretation of our findings and restrict insights into potential phenotype-specific management strategies. Future studies should incorporate HF phenotyping to provide a more comprehensive understanding of the interplay between NVAF and HF.
Additionally, the study did not assess the appropriateness of dosing for DOACs or collect INR data to calculate the time in therapeutic range (TTR) for patients treated with VKAs. These metrics are critical for evaluating anticoagulation quality and clinical outcomes but were beyond the scope of this study. Future research should include these measures to provide a more comprehensive evaluation of anticoagulation management in patients with NVAF.
The relatively short follow-up period of 12 months was insufficient to fully assess long-term clinical outcomes. Future research should include a more representative patient sample from both private and public healthcare settings, alongside extended follow-up durations, to provide a comprehensive understanding of NVAF management across diverse healthcare contexts in Egypt.

Comments (0)