
Remember me
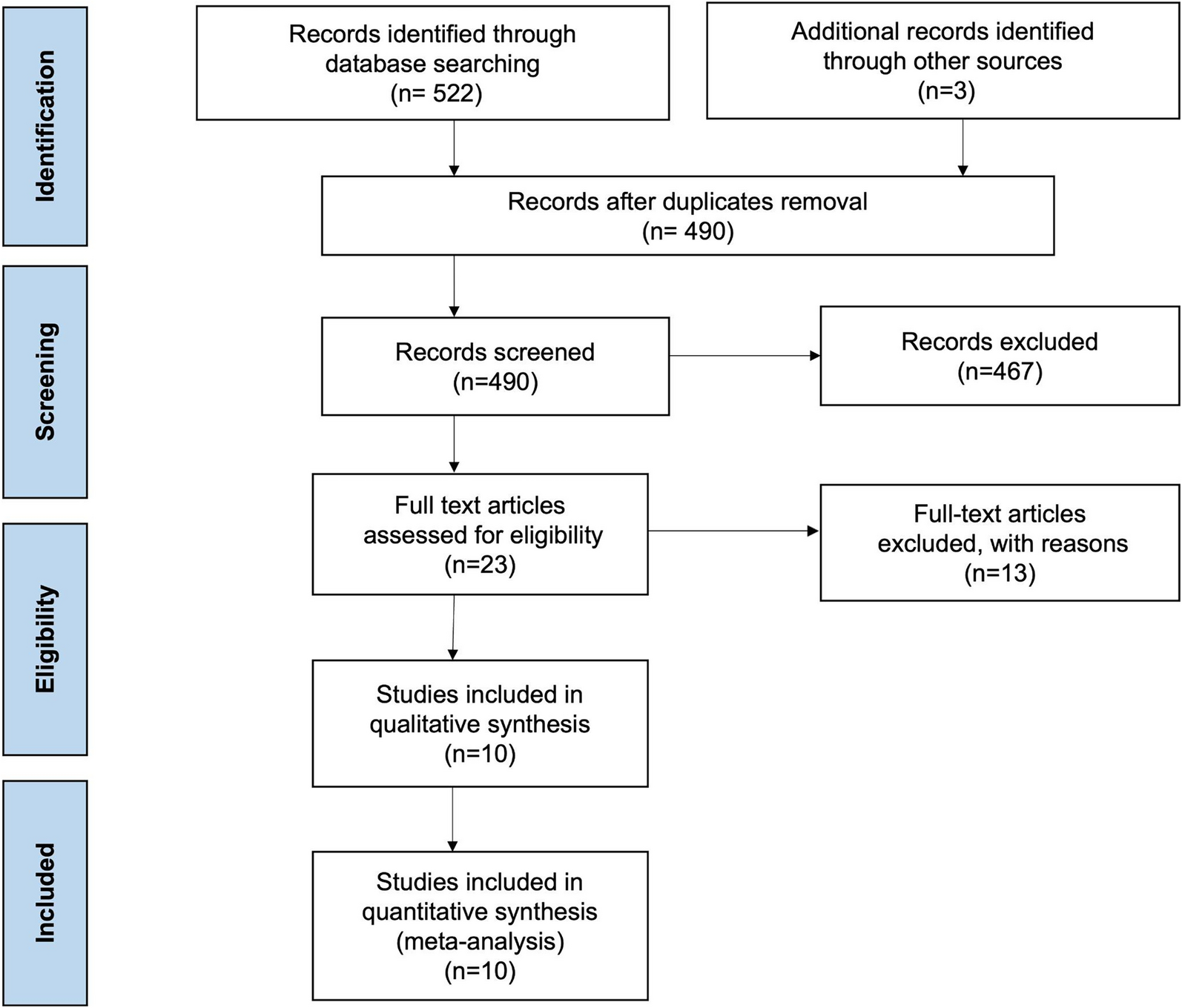
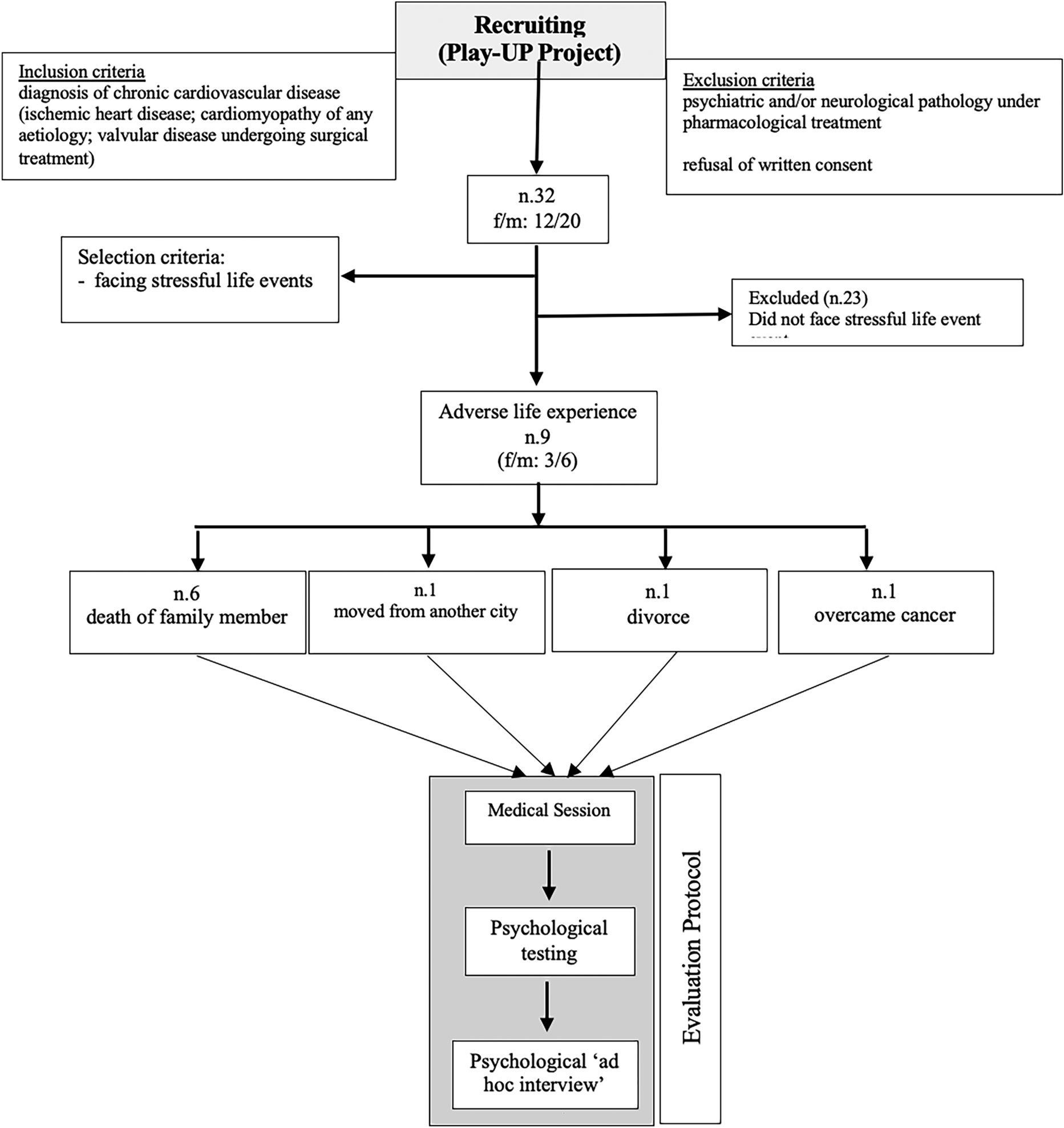
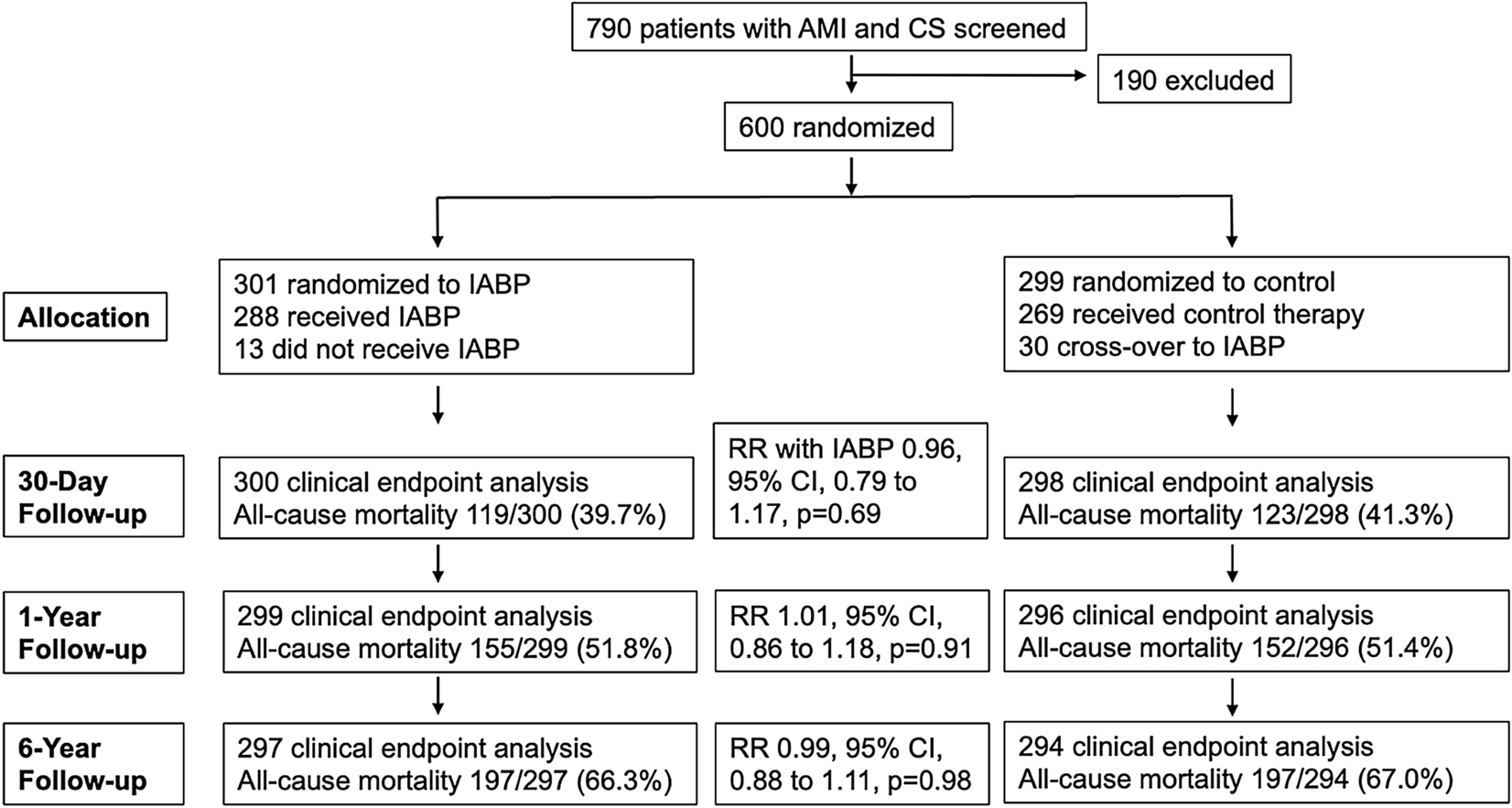
Participants in this study were selected from a wider sample of the ongoing Play-UP study protocol aimed at analyzing the relationships among allostatic load modelling, lifestyle and cardiological risk factors. Nine of 32 patients from the Play-UP Project were included in the study because of their exposure to stressful life experiences. During the research period from March to April 2024, nine patients with cardiomyopathy, ischemic cardiomyopathy, and HF were selected for this mixed-method study. Figure 1 shows a flowchart of the patient-selection process.
Fig. 1 Characteristics of the Participants: Quantitative Analyses
Characteristics of the Participants: Quantitative AnalysesThe average age of participants (coded A to I) was 72.5 years old (DS ± 7.5) (range 58–80 years). There were six male participants and three female participants; seven patients were completely independent of ADLs, and two reported being slightly dependent on their wives, especially in the management of medication and cardiological follow-ups scheduled every 6–8 months (Tables 2 and 3).
Table 2 Demographic characteristics of participantsTable 3 Medical parametersPatients were assessed based on demographics and lifestyle variables (age, sex, marital status, educational level and BMI), as well as comorbidities (e.g., diabetes mellitus, hypertension, chronic obstructive bronchopneumonia, atrial fibrillation, and cancer). Laboratory test results (high-density lipoprotein cholesterol, lipoprotein, triglycerides, blood pressure, albumin-to-creatinine ratio, and natriuretic peptides) and clinical parameters (i.e., blood pressure and heart rate) were reported. Medications (i.e., ACE-inhibitors, beta-blockers, antihypertensives, diuretics, lipid-lowering agents, neprilysin inhibitors and gliflozins) have also been reported. A list of diagnoses, comorbidities and clinical data is presented in Tables 2 and 3: almost all patients showed hypertension as a comorbidity, while a few patients also had diabetes and chronic obstructive broncho-pneumopathy.
Almost all patients also showed CV disease from relevant time (> 4 years of disease) and they were undergoing polypharmacological therapies demanding medical treatment regimen; NYHA classification evidenced four patients had no limitations of physical activity, three suffered slight limitation of physical activity in the presence of fatigue and two showed marked limitation of physical activity. Regarding anthropometric factors (WHR index), six patients were at high risk of cardiovascular disease. Patients were treated according to guideline recommendations [27]. Patients discussed treatment options with cardiologists; specialists prescribed the therapies, how to take them and information about side effects as well as alternative treatments. All patients accepted the treatments, and to develop adherence, cardiologists planned a check to favor complex treatment regimens in 2 weeks. Follow-ups were scheduled every 6–8 months.
Cognitive reserve (by CRIq) and risk of cognitive decline (by MMSE) were evaluated (Table 4). The CRIq scores showed that one patient reported a high level of cognitive reserve, one reported a low level and seven reported a medium level. Using MMSE, we identified only two patients at risk of mild cognitive impairment. The combined MMSE and CRIq indices highlighted the resilience of patients because they showed high ADL function (Table 2). Finally, self-perception of QoL was high: one patient reported a reduced QoL perception related to living alone and suffering from affective separation (divorce) and another reported a decrease in cancer diagnosis and treatment.
Table 4 Psychological parametersQualitative AnalysesThe interviews were based on five themes: (1) emotional triggers, (2) family and social support, (3) impulsiveness, (4) therapeutic relationship with the cardiologist, and (5) QoL. Table 5 presents the themes and related quotes from the interviews.
Table 5 Details of interview: themes, questions and quotesTheme 1—Emotional TriggerParticipants’ responses to the interview were as follows: when asked, ‘Was there an emotional trigger for your disease?’ Nine reported their own CV condition related to the emotional trigger regarding the adverse life experience: six patients witnessed the death of a family member (e.g., father, daughter, husband), one patient described the divorce from his wife as very painful, one moved to another city for economic reasons and one reported the impact of the cancer diagnosis. Patients perceive specific life experiences as negative outcomes for their well-being that compromise their heart health.
To the question ‘Do you perceive yourself as frail?’ all patients described themselves as frail. Even family members who were present believed that these patients were frail. People with HF felt frail in relation to life experiences associated with a high level of negative emotions; almost all had dealt with the death of family members and reported a decrease in physical and mental well-being. Analyzing the quote, patients referred to experiencing mental discomfort directly linked to physical impairment (health failure or cardiopathy). Our patient reported a lived adverse experience as a precursor to CV issues.
Theme 2—Family and Social SupportFamily and social support are buffering factors for frailty. Cardiovascular patients experience difficulty in managing and caring for their health; therefore, family and/or social support, as well as healthcare providers, have emerged as important. Particularly, intimate relationships such as marriage, family members and/or friends are integral aspects of behavioral or psychosocial influences on the development, course, impact and management of cardiovascular disease. Smith [28] highlighted that cardiovascular patients living with partners generally seemed more adaptively engaged in healthcare than single patients: the author highlighted the relevant role of caregiver/partner engagement in the cure of the patient and more in the understanding of emotional distress, as their expressions of distress may modulate patients’ own fears and concerns. Furthermore, the adjustment to coping with the disease and related care could present negatively in both patients and partners, who each may have different views of the disease. Participant A reported that his family did not know about his check-up and the possible surgery in a few months; he sustained that his wife was unable to manage her distress for his health, so he preferred not to say anything. Health behaviors as prevention targets result in affective dynamics. Finally, intimate relationships are an important aspect of patients’ adjustment to stressful events caused by cardiovascular disease and its treatment.
To the questions ‘What was the help from your family like? and ‘What was the help from your friends’ companionship like?’ patients A, C, G, I, and H responded that they received family or social support for their daily or leisure activities (Table 5). Evidence of the importance of family and social support is typically associated with a reduced risk of cardiovascular disease, improved prognosis, more effective health-behavior changes and patient management and maintenance. In contrast, strained and disrupted relationships can exacerbate cardiovascular risk and complicate patient care. Family and social support appeared to have negative/positive buffering effects on the interactive process between social networks and individuals with cardiovascular disease in maintaining self-care behaviors that enhance optimal health.
Theme 3—ImpulsivenessImpulsivity is a psychological dimension based on the inability to conform to context or consequences and is a predictive dimension of maladaptive behaviors. In cardiology patients, the behavioral component could be a predictive factor for poor prognosis of cardiology events. Our patients reported fairness in reducing their QoL, showing relevant impulsive thoughts of intrusive thinking about difficulties in concentration. Moreover, maladaptive behaviors with high impulsivity can favor unhealthy behaviors and increase the risk of adverse events. Leroy et al. [29] evidenced that impulsivity is related to individual temperament and moderated by emotional characteristics, highlighting that impulsivity could be either a pejorative or protective risk factor. Participant B reported to have intrusive thinking regarding the dead daughter (‘My intrusive thought is my daughter. How can I not think about it? I’ve tried every which way, but I can’t. My thoughts automatically go there…’), as Participant E sustained not having enough self-control (‘Sometimes… But sometimes not… It depends on how I feel at that moment. But most of the time, it does’). Few patients reported good self-control and low impulsivity. Our participants with intensive emotional triggers tended to feel impulsive and, following Leroy’s [29] suggestions, this could indicate a persistent risk of low adherence to healthy behaviors and coping with medical advice. Providing personalized and patient-centered care based on patient engagement could be a promising cure setting that buffers the impact of the convergence of symptoms between CVs and frailty, facing challenges in determining higher adherence to therapeutic solutions.
Theme 4—Therapeutic Relation with CardiologistClinical practice and scientific evidence have highlighted the need to engage patients in clinical relationships to manage the burden of cardiovascular risk of adverse events [30, 31]. This finding appeared to be salient for our participants. Participant B revealed the human relationship regarding own fears, ‘I feel comfortable with telling him everything’. Participant I talked about the fear of change in the management of the disease (‘When I don’t understand something, he knows how to explain it to me and that calms me down … he is always very helpful, calm and attentive’) and the ability of the cardiologist to overcome and make it more suitable considering being in a new care scenario. Cardiologists appeared to apply their technical skills better using interpersonal skills to build rapport and address fears. Building trust represents almost all features needed to improve and manage patient outcomes. Feeling ‘cured and cared for’ is a psychological dimension detected in spontaneous talking of patients and seemed to be a pillar in their health management. Considering Gringras’s [32] suggestions, all highlighted that the human link with cardiologists featuring a therapeutic relationship is basilar in the quality of patient experience. In treatment compliance, the connection between an alliance with doctor and patient medication adherence appeared salient to cure patients: according to the literature [33], medication non-adherence is prevalent among patients with chronic diseases and is influenced by patient-, medication- and illness-specific and contextual factors.
Theme 5—Quality of LifeThe self-perception of our patients’ QoL was good; they felt cured by medical staff, supported by suggestions. Additionally, pharmacological treatments helped them manage their frailty efficiently. Even by VAS evaluation, the score was high; Participant E appeared aware of their own cognitive decline related to living alone and economic issues. All medical evaluations highlighted physical weaknesses that were supported by polypharmacological treatments. Although they were almost autonomous, they needed help from caregivers and felt satisfied with the balance between clinical risk and QoL.
Comments (0)