While current standard pharmacologic therapies for obstructive HCM offer symptomatic relief, they do not address the underlying pathophysiological mechanisms of HCM. Mavacamten has been shown to improve clinical symptoms and health status in Chinese patients with symptomatic obstructive HCM, but data are lacking on whether these improvements were accompanied by changes in important disease-related markers of cardiac structure and diastolic function in these patients. This analysis of echocardiographic assessments of Chinese patients with obstructive HCM in EXPLORER-CN demonstrated that mavacamten treatment for 30 weeks led to clinically meaningful improvements in cardiac structure and function assessed by transthoracic echocardiography imaging, including LAVI, LVMI, LVED interventricular septal thickness, LVED posterior or maximal wall thickness, and E/e′ ratio. Of note, these improved parameters represent key pathophysiological features of obstructive HCM, thus adding further support for the mechanism of action of mavacamten in addressing the underlying pathophysiology of the disease. Improvements in echocardiographic measures of cardiac diastolic function have also been noted in the VALOR-HCM trial, which showed that mavacamten reduced the need for septal reduction therapy at week 56 [22]. Importantly, our findings expand the evidence of a favorable treatment effect of mavacamten on echocardiographic changes in a diverse population, including Chinese patients, in whom poor CYP2C19 metabolizers are more prevalent and body mass index tends to be lower compared with global patients.
Abnormalities in mitral valve SAM are a key feature of obstructive HCM, and the degree and severity of SAM are associated with LVOT obstruction, clinical symptoms, and outcomes in HCM [23]. Considering that mitral valve SAM is a key mediator of the dynamic LVOT gradient seen in obstructive HCM, the benefit of mavacamten in resolving SAM is particularly relevant for patients with obstructive HCM. After 30 weeks of treatment with mavacamten, the proportion of patients achieving complete resolution of mitral valve SAM was three times larger than in the placebo group (23.1% vs. 7.4%). In line with SAM resolution, mavacamten-treated patients had better resolution of MR than those receiving placebo, with all 12 patients who presented with moderate MR at baseline experiencing improvement to mild or trace MR by week 30, while four patients in the placebo group remained with moderate MR status at week 30 (seven patients had moderate MR at baseline). In keeping with the beneficial effects of mavacamten in SAM resolution, significant reductions in LVOT gradient at rest and during Valsalva have been observed with mavacamten versus placebo [10]. Despite the remarkable reductions in LVOT gradients, cardiac output remained unchanged following mavacamten treatment. The incidence of treatment-emergent adverse events was also similar between the mavacamten and placebo groups, and no patients had LVEF < 50% or developed HF at week 30, as reported previously [17], suggesting that there are no excessive reductions in LVOT gradients leading to low-output symptoms.
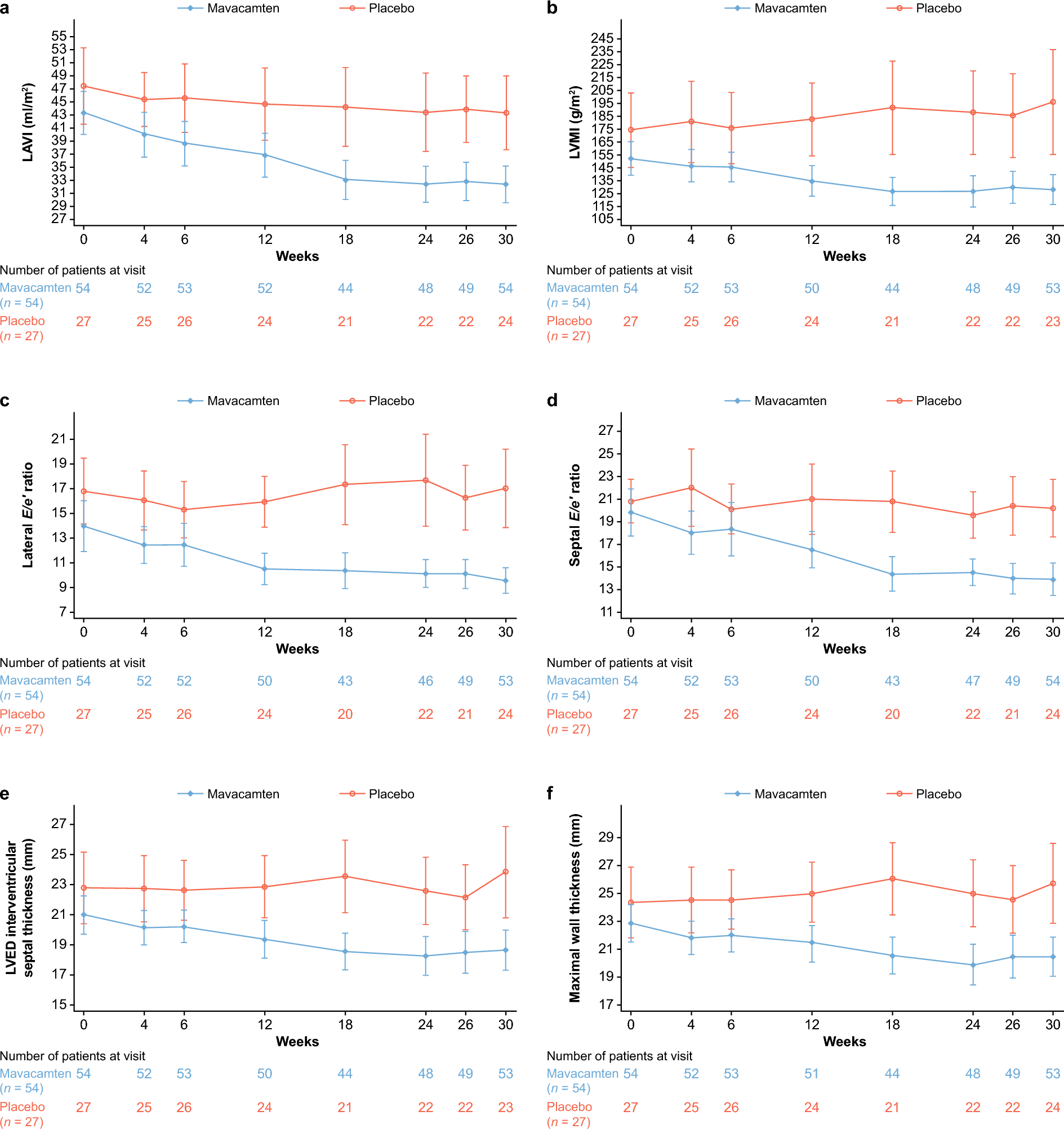
Following the resolution of SAM and relief of LVOT obstruction, improvements in LV filling pressure can be expected with improved hemodynamics. E/e′ ratios, which are indicators of diastolic function associated with instantaneous LV filling pressure [24], were improved with mavacamten in our study: both ratios of lateral E/e′ (9.6) and septal E/e′ (13.9) in the mavacamten group were reduced to within normal range while the corresponding values in the placebo group (20.2 and 17.0, respectively) remained elevated at week 30 (average E/e′ ratio > 14 is considered abnormal) [25]. These changes are consistent with the reductions seen with mavacamten treatment in the global population in the EXPLORER-HCM (– 3.8 and – 3.5 for lateral and septal E/e′, respectively) and the VALOR-HCM (− 3.3 for average E/e′) trials [16, 22]. Another indicator of LV filling pressure, LAVI, which was elevated at baseline (mean, 43.3 and 47.5 ml/m2 for the mavacamten and placebo groups, respectively), was reduced to a mean of 32.4 ml/m2, a level considered to be within the normal range [25], in response to mavacamten treatment, while LAVI remained elevated in the placebo group (mean, 43.4 ml/m2). In the global populations, mean change in LAVI was – 7.5 ml/m2 at week 30 in the EXPLORER-HCM trial and − 5.2 ml/m2 at week 16 in the VALOR-HCM trial [16, 22]. Furthermore, the LSM reduction in LAVI of 11.7 ml/m2 with mavacamten is consistent with a mean reduction of 17.4 ml/m2 assessed by CMR imaging following mavacamten treatment in EXPLORER-CN [17]. Of note, a favorable effect of cardiac myosin inhibition in cardiac remodeling has also been shown in the SEQUOIA-HCM CMR substudy [26]. Taken together, the echocardiographic changes seen are consistent with the global populations in the EXPLORER-HCM and VALOR-HCM trials [16, 22], indicating that the beneficial treatment effects of mavacamten in improving the pathophysiology of obstructive HCM also extends to the Chinese population.
Improvements in the echocardiographic parameters mentioned above following mavacamten treatment were likely mechanical consequences of mavacamten’s inhibitory effect on actin–myosin cross-bridges. Suppression of cross-bridge formation can potentially reduce LV stiffness and improve LV compliance, thereby leading to lower filling pressures. Mavacamten was also shown to promote detachment of actin-myosin cross-bridges in preclinical biophysical studies, resulting in improved diastolic relaxation [27]. In addition, inhibition of myosin adenosine triphosphatase activity by mavacamten was shown to decrease sarcomere power and force generation in preclinical animal models, thus alleviating the hypercontractile state [12, 28, 29], which is desirable for improving hemodynamics in patients with obstructive HCM. The ensuing reduction in hypercontractility may contribute to the resolution of SAM and LVOT obstruction, thereby improving LV filling pressure, consistent with the clinical finding of reduced E/e′ ratio seen with mavacamten.
As elevated E/e′ ratios and LAVI were predictive of adverse long-term outcomes, including HF, AF, stroke, and sudden cardiac death [9, 9,30,31,32,33,34,35], improvements in these measures and other parameters related to LV mass and wall thickness could potentially have long-term clinical benefits such as a reduction in cardiovascular events, though this would require validation with longer follow-up. On the other hand, the potential to reverse these markers of diastolic function to within normal range with just 30 weeks of mavacamten treatment holds important implications for HCM management. Of note, the curves for these indices of LV filling pressure separated between the treatment groups as soon as week 4; this separation was sustained to week 30, which corresponds to the separation of curves seen with LVOT peak gradient at rest or during Valsalva. In addition, improvements in these indicators were observed regardless of the NYHA functional status of patients at baseline, although the small sample size in each subgroup warrants caution in interpretation of results.
In the present study, reductions in selected echocardiographic measures such as LVOT gradients at rest or with Valsalva and LAVI appeared to be correlated with reductions in NT-proBNP, consistent with findings in the global EXPLORER-HCM echocardiographic substudy [16]. NT-proBNP is a known indicator of cardiac wall stress, which has been shown to be predictive of adverse outcomes and deaths in patients with HCM. While other HCM therapies such as metoprolol and disopyramide reduced LVOT gradients and improved NYHA functional class in patients with obstructive HCM, the treatment effects on NT-proBNP were minimal [36, 37]. In addition, the correlations between improvements in LAVI and E/e′ with a reduction in NT-proBNP levels suggest that mavacamten has a beneficial effect through reducing LV filling pressure that accompanies relief of LVOT obstruction.
Beyond what has been reported previously, we also analyzed the association between key echocardiographic parameters and the patient-reported health status indicator of KCCQ-23 OSS as well as changes in echocardiographic measures stratified by NYHA class in this study. Previously, mavacamten was associated with a greater improvement in KCCQ-23 OSS across all KCCQ subscales versus placebo, with more patients achieving ≥ 10 points increase in KCCQ-23 OSS with mavacamten [38]. In addition, decreases in LVOT gradient at rest or with Valsalva and LVED interventricular septal wall thickness have all been shown to be associated with improved KCCQ-23 OSS in patients with obstructive HCM [39]. Our findings of moderate associations between KCCQ-23 OSS improvement with reductions in LVED interventricular septal thickness and LVOT gradient at rest or with Valsalva in the Chinese population are in line with those observed in the global EXPLORER-HCM trial. Taken together, these findings suggest that the reduction of LVOT obstruction, with greater reduction following mavacamten treatment versus placebo, is associated with better quality of life for patients with HCM.
Limitations include relatively small sample size and short duration of study. As only patients with NYHA class II–III were included due to study eligibility criteria, our findings are not generalizable to other populations of HCM. The study only included the use of beta-blockers as a stratification factor, so there may be other potential confounders such as prior septal reduction therapy or the presence of AF that might have influenced results. Also, accurate assessment of MR is limited due to its highly erratic nature in obstructive HCM. In addition, there may be potential variabilities inherent in echocardiographic measurements, although echocardiography was conducted according to standardized protocols and analyzed at a central laboratory.

Comments (0)