In this study, we report the findings of one of the largest AH screening initiatives in Kazakhstan. Key findings include: (1) a notable decline in the proportion of participants who had never had their BP measured (27% in 2021 vs. 12% in 2023); (2) a high AH prevalence (37–45%), with key risk factors being older age, male sex, and high BMI; (3) a trend towards increasing AH awareness, from 50% in 2021 to 66% in 2023; (4) a significant gap in BP control, whereby although 68–91% of aware individuals were on treatment, fewer than 50% achieved BP < 140/90 mmHg and only 15–16% met the stricter < 130/80 mmHg target.
Consistent with our findings, 32% of participants in the 2019 global MMM study reported having BP measured for the first time [10]. A global correlation was observed between BP measurement rates and national income [10]. The decline in first-time BP measurement in our study may reflect differences in study sites, as screenings in 2022–2023 were limited to Almaty, where healthcare access is higher [11].
The 37% AH prevalence in Kazakhstan’s MMM 2021 survey aligns with global MMM estimates (35%) [6] and the World Health Organization’s 2023 AH report (42%) [12]. Similar to previous MMM campaigns [6, 10, 13, 14], we confirmed higher BP in men, older adults and those with high BMI. However, the findings in global data, the findings of Kazakhstan’s MMM 2021 survey found that smoking and alcohol consumption were not significantly associated with BP, possibly due to underreporting.
AH prevalence in Almaty (45%) was significantly lower than the 70% reported in Nur-Sultan in 2012–2013 [9]. While national reports suggest increasing AH prevalence [5], our findings imply that earlier estimates may have been influenced by selection bias, as in the 2012–2013 study, BP was measured only in outpatient clinics in Nur-Sultan.
In line with global MMM 2021 data, approximately 50% of hypertensive participants in 2021 were aware of their condition [6]. Awareness often correlates with education and socioeconomic status [9], explaining regional disparities [6]. The rise in awareness (to 70%) in 2022–2023, when screenings were conducted in Almaty, and the high awareness in Nur-Sultan (91%) in 2012–2013 [9], may reflect differences in healthcare access and health literacy [15].
Overall, the findings of our study are consistent with the results of the global MMM 2021 and Nur-Sultan studies in that while the majority of AH-aware participants received hypertensive medication, only up to half of those on antihypertensive therapy were controlled to the conservative BP target of < 140/90 mmHg. When we used the lower BP target of < 130/80 mmHg as the definition of control, which more accurately reflects current guidelines [16,17,18,19,20], the control rate among those treated in 2021–2023 decreased to 15–16%. Factors that could be contributing to low rates of BP control include poor adherence to antihypertensive therapy, lack of general knowledge about the importance of BP control and failure of healthcare providers to intensify treatment to achieve BP control as appropriate.
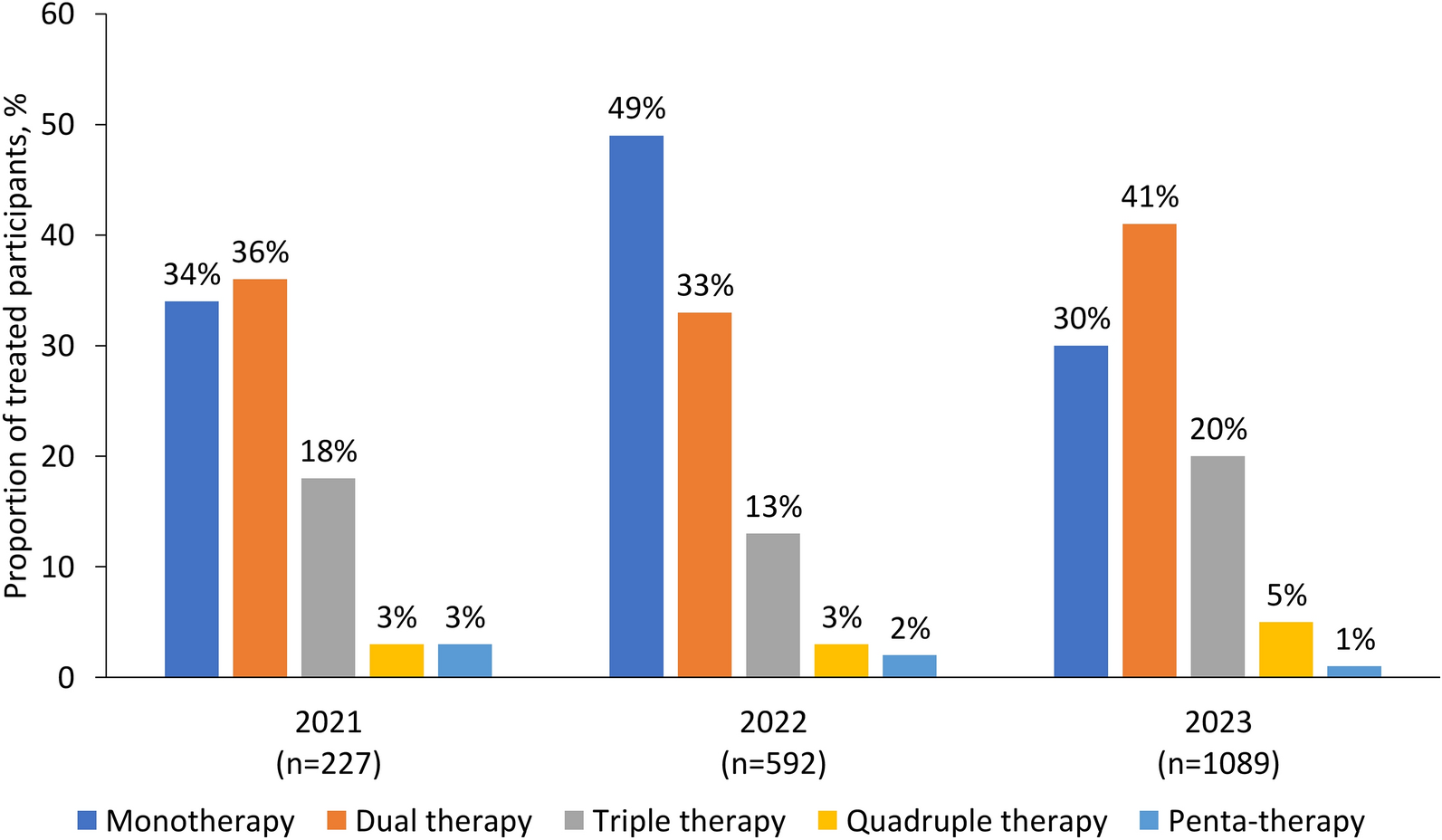
Poor treatment adherence was identified as a problem in this study, particularly in younger hypertensive participants. This may reflect limited access to free medications and lack of knowledge about the risks of high BP and the importance of taking medication as prescribed to control BP. Furthermore, of those taking medication, more than one-third were only on a single therapy in all 3 years of the survey, despite the latest European Society of European Society of Hypertension (ESH) guidelines recommending initiation of drug treatment with two antihypertensive medications to achieve effective BP control [20]. As pointed out in the global MMM survey [6], there is significant scope for improvement of BP control with single-pill combination therapies as advised by AH guidelines in use during the 3 years of the campaign [18, 20].
The study highlights significant gender and age-related disparities in AH awareness and BP control. Awareness levels were consistently higher among female patients compared to male patients, with a significant upward trend over the years. However, despite this improvement, BP control remained suboptimal, particularly among men and younger adults. Age was strongly associated with awareness, with older individuals demonstrating significantly higher awareness and better BP control than younger age groups. Nevertheless, strict BP control (< 130/80 mmHg) remained low across all groups, underscoring the need for more aggressive intervention strategies to improve adherence to treatment and BP management.
Furthermore, findings suggest that barriers to effective secondary prevention—including limited access to high-quality antihypertensive medications under the state-guaranteed benefit package in Kazakhstan—may contribute to inadequate BP control. The predominance of low-quality generic drugs distributed through public healthcare services could explain the persistent treatment gaps, especially among high-risk patients with a history of MI, stroke, and diabetes.
These results emphasize the need for improved access to effective antihypertensive medications, better patient education programs and enhanced treatment strategies tailored to vulnerable populations. Future efforts should focus on addressing non-adherence due to medication unavailability, affordability issues and the need for stricter clinical follow-up to optimize AH control and reduce cardiovascular risk.
This study had several limitations. Most importantly, the true prevalence of AH in Kazakhstan could not be evaluated because a nationally representative sample was not targeted. Kazakhstan has 14 regions, but the study included only four cities from the south, center and east of country in 2021, and only one large city in 2022 and 2023. Further nation-wide studies that include rural areas are needed. A study focused solely on urban populations may not accurately reflect the overall AH burden, as rural residents experience different healthcare access, lifestyle factors, and treatment barriers. Urban populations generally have better healthcare access, higher health literacy level and more frequent screenings, leading to greater awareness and treatment adherence. However, city dwellers also face higher stress levels, have relatively sedentary lifestyles and consume higher quantities of processed foods, which may contribute to AH. City dwellers benefit from better medication availability and specialist care, whereas rural populations struggle with limited access, long travel distances and higher costs, leading to lower treatment rates. Also, AH was identified using a single set of three measurements taken on a potentially high-stress occasion. This is not recommended diagnostic practice [19, 20], and may lead to a high proportion of false positives [14]. Additionally, half of the BP measurements were taken in medical settings, which may result in the self-selection of a greater proportion of participants with AH [13]. It is therefore possible that our results overestimated AH prevalence due to white coat AH or stress, and that it missed increased BP that in some can only be found during continuous monitoring (masked AH). Nonetheless, the primary aim of the study was to raise awareness of the importance of annual BP measurement in a large cohort of people. We were able to identify individuals with increased cardiovascular risk and suspected AH, who could be further referred for 24-h BP monitoring.

Comments (0)