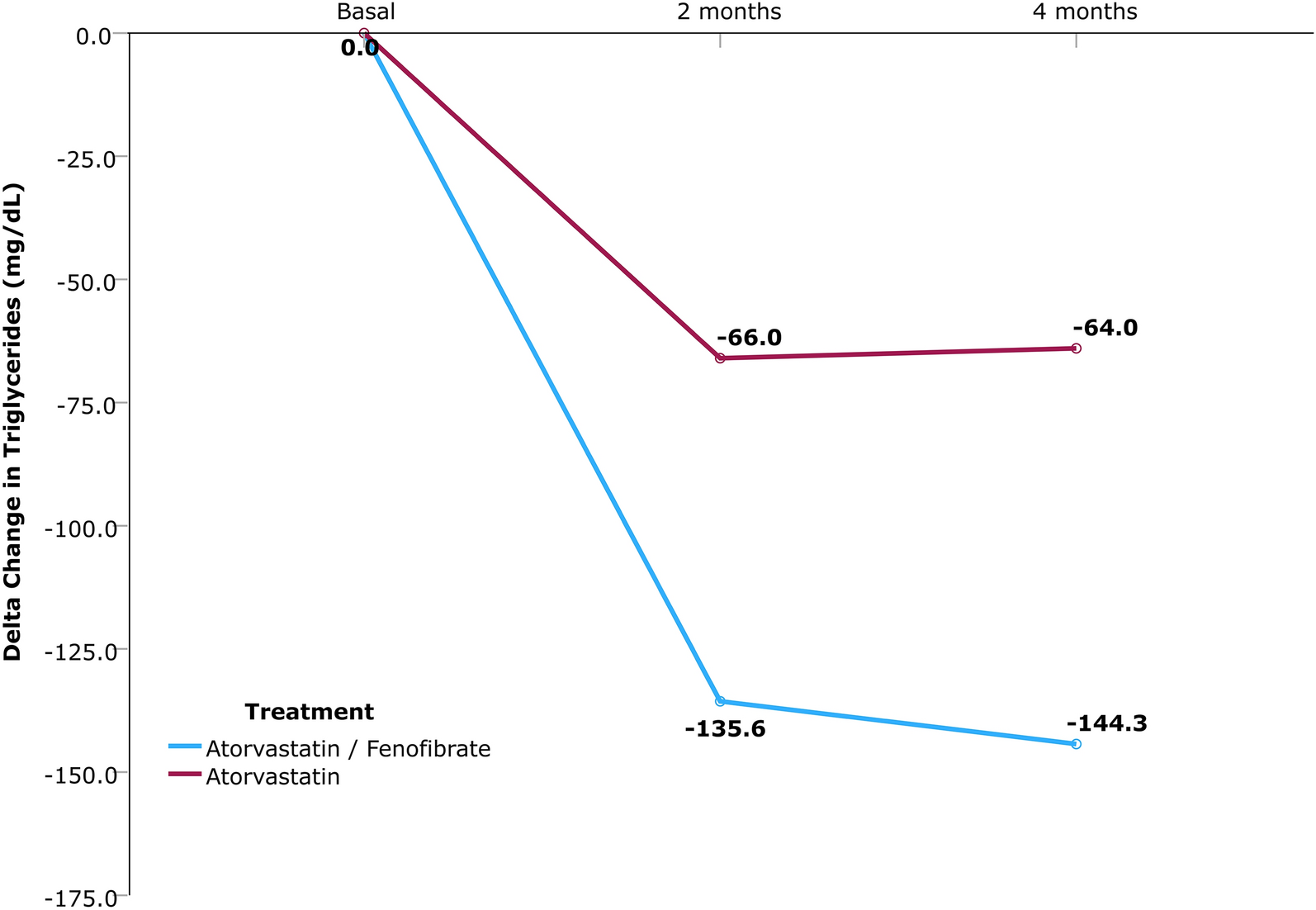
The analysis of the results from this confirmatory clinical study on the efficacy and safety of the FDC of atorvastatin/fenofibrate (G_FDC) versus atorvastatin (G_M) provides solid scientific evidence of the advantages of using a combination therapy in T2DM. The reduction in TG (∆ of change) after 4 months for the atorvastatin/fenofibrate group was −144.3 mg/dL, while for the atorvastatin group it was −64.0 mg/dL (p = 0.006), with a percentage change of −43.1 vs. −22.8 (p = 0.008), respectively. This outcome was replicated in the predictive cardiovascular risk indices (∆ of change) between the atorvastatin/fenofibrate group of treatment and the atorvastatin group: in the TG/HDL index −3.9 ± 4.6 vs. −1.5 ± 2.9, (p = 0.015), and in the TG/glucose index −0.7 ± 0.5 vs. −0.3 ± 0.4, (p = 0.003). The use of the atorvastatin/fenofibrate combination demonstrated a favorable safety profile without any increase in adverse events.
As previously described, T2DM is a metabolic disorder that frequently predisposes individuals to cardiovascular diseases (CVD), with lipid abnormalities being a common condition [6]. According to Hirano’s publication on the pathophysiology of dyslipidemia in patients with diabetes, also referred to as “diabetic dyslipidemia,” it is associated with an atherogenic lipid profile (hypertriglyceridemia, normal or slightly elevated LDL-C but with an increase in small dense LDL, reduced HDL-C and elevated non-HDL cholesterol) that increases the risk of cardiovascular disease [21]. Moreover, this condition is associated with cardiovascular diseases such as stroke, acute myocardial infarction, coronary artery disease, and congestive heart failure, which are the leading causes of death in these patients [22].
In our study, as part of the inclusion criteria for patients, the presence of parameters including total cholesterol, LDL-C, non-HDL cholesterol, and TG above the normal range were included. These were measured at the end of the treatment to evaluate the efficacy of the FDC therapy in comparison with baseline measurements, as reported in several clinical studies. Accordingly, our results showed an overall improvement in the lipid profile of patients treated with the atorvastatin/fenofibrate combination throughout the follow-up, with reductions in parameters such as TG, LDL-C, total cholesterol, and non-HDL cholesterol. All final parameter results were compared with baseline measurements within the group and were found to be both clinically and statistically significant.
The findings in this study align with those reported in the literature. The use of the combination of both drugs has proven effective in improving the lipid profile in patients with T2DM and dyslipidemia. Additionally, the superiority of atorvastatin/fenofibrate FDC compared to monotherapy has been proposed [20, 23,24,25].
Lella et al. [20] conducted a prospective, open-label clinical trial in patients with T2DM and hyperlipidemia (total cholesterol > 200 mg/dL, TG > 150 mg/dL, LDL-C > 100 mg/dL, and HDL-C < 40 mg/dL). In this study, the atorvastatin 40 mg and fenofibrate 145 mg CDF was compared with atorvastatin 40 mg over 12 weeks in 60 patients, assessing its effects on lipid profiles. After 12 weeks, the reduction in total cholesterol, TG, and very low-density lipoprotein (VLDL) cholesterol was greater in the atorvastatin/fenofibrate group than in the atorvastatin-only group.
In another study conducted by Davidson et al. [25], a multicenter, double-blind, randomized, parallel-group phase IIa clinical trial was conducted in 220 patients with dyslipidemia (non-HDL cholesterol > 130 mg/dL and TG ≥ 150 but ≤ 500 mg/dL). The atorvastatin 40 mg and fenofibrate 100 mg FDC was evaluated against atorvastatin 40 mg or fenofibrate 145 mg for 12 weeks. The primary efficacy endpoints were the mean percentage changes from baseline to week 12 in non-HDL cholesterol, HDL, and TG, concluding that patients treated with the CDF showed improvements in HDL cholesterol and TG levels. As described above, the results are consistent with those obtained in our study, emphasizing that the evidence in the literature supports the value of the FDC atorvastatin/fenofibrate in improving the lipid profile not only of patients with T2DM and mixed dyslipidemia but also of those with isolated lipid abnormalities.
Additionally, it is important to mention that various clinical studies have reported that hypolipidemic therapy plays a key role in reducing mortality in these patients, where statins are the most commonly used drugs to lower LDL-C and cardiovascular risk. However, in diabetic dyslipidemia, residual risk is associated with elevated TG levels and low HDL-C levels, which is why additional hypolipidemic therapies, such as fibrates, are required for more significant cardiovascular risk reduction [26].
Based on the relevance of hypolipidemic therapy and the importance of using additional therapies, this study also evaluated the TG/glucose and TG/HDL indices, showing the advantage of FDC atorvastatin/fenofibrate at 2 and 4 months of follow-up. These reductions in the indices indicate an improvement in insulin resistance and, consequently, a potential decrease in cardiovascular risk [7, 27, 28].
Specifically, in the case of patients with T2DM, several investigations including the FIELD (Fenofibrate Intervention and Event Lowering in Diabetes) [24] study and the ACCORD (Action to Control Cardiovascular Risk in Diabetes) [23] study have evaluated the effect of therapy with fibrates, statins, or their combination on various biochemical markers and cardiovascular disease, demonstrating a substantial improvement in the lipid profile. In the long-term follow-up study ACCORDION, where patients from the ACCORD study were followed, a reduction in all-cause mortality was observed in the group treated with fenofibrate + statins [hazard ratio (HR): 0.68; 95% CI: 0.52–0.88], supporting the use of fibrates as complementary therapy to statins in reducing cardiovascular risk in patients with diabetes and dyslipidemia [29, 30].
Recent epidemiological studies have primarily highlighted the positive effects and clinical benefits of statin/fenofibrate therapy in patients with T2DM.
Hong et al. [31] conducted a nationwide propensity-score-matched cohort study investigating the effects of fenofibrate combined with statin therapy on all-cause mortality and atherosclerotic cardiovascular disease (ASCVD) in 110,723 patients with diabetes, triglyceride (TG) levels ≥ 150 mg/dL, and no prior ASCVD diagnosis. Patients using statins plus fenofibrate were matched 1:1 with those using statins alone. Over a mean follow-up of 4.03 years, the fenofibrate/statin group showed significantly lower risk of all-cause mortality (HR 0.71; 95% CI 0.68–0.74) and ASCVD events (HR 0.89; 95% CI 0.85–0.93), including myocardial infarction (HR 0.878; 95% CI 0.827–0.933) and stroke (HR 0.901; 95% CI 0.848–0.957), compared with the control group. These benefits were consistent in patients with TG levels between 150 and 199 mg/dL and particularly in those with elevated LDL-C.
Ku et al. [32] performed a nationwide population-based retrospective observational study to evaluate the preventive effects of fenofibrate on lower extremity amputation (LEA) and peripheral arterial disease (PAD) in patients with T2DM. Using data from the Korean National Health Insurance Service Database (2009–2012), 22,984 statin/fenofibrate users were matched 1:4 with 91,936 statin users. Over a median follow-up of 7.6 years, statin/fenofibrate use was associated with significantly lower risk of LEA and PAD (HR 0.81; 95% CI 0.70–0.94), LEA alone (HR 0.76; 95% CI 0.60–0.96), and PAD alone (HR 0.81; 95% CI 0.68–0.96). No significant differences were observed in safety outcomes, including acute kidney injury and rhabdomyolysis. The benefits remained consistent across age, gender, and lipid profiles.
Concerning the safety profile of the atorvastatin/fenofibrate combination, our study demonstrated no difference against atorvastatin monotherapy; most of the adverse events were mild and moderate, with no severe adverse events reported. This is consistent with the safety data reported in the aforementioned studies [20, 25, 33], confirming that the safety profile of the combination is favorable.
Furthermore, it is important to highlight that the treatment evaluated in this study is supported by previous publications in various guidelines and expert consensus on managing dyslipidemias. The American Association of Clinical Endocrinologists (AACE) and the American College of Endocrinology (ACE) recommend statins as the first-line treatment for lowering cholesterol and advocate for combination therapy with other agents, such as fibrates, particularly due to their triglyceride-lowering effects [11]. Similarly, the European Society of Cardiology (ESC) and the European Atherosclerosis Society’s Guidelines for the management of dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk emphasize statin therapy and recommend adding another lipid-modifying agent, such as fibrates, for patients who are intolerant to statins or who fail to therapeutic goals with statin monotherapy, especially when dyslipidemia is characterized by elevated TG levels [9].
In addition to the widely studied efficacy of the combination therapy, the cost–benefit of these drugs in treating dyslipidemia and preventing vascular disease has also been evaluated. According to the AACE guidelines for managing dyslipidemia and preventing cardiovascular risk, [34] non-pharmacological interventions are the most cost-effective options for preventing cardiovascular disease. Unfortunately, in many cases, they fail, and pharmacological intervention is the most recommended option, especially for individuals with moderate to high cardiovascular risk. Among pharmacological interventions, statins have been shown to be cost-effective in preventing primary and secondary cardiovascular events in individuals with moderate to high risk, and fibrate therapy has also been reported as cost-effective as monotherapy and in combination therapy to reduce TG and increase HDL-C [34].
Finally, as discussed earlier, treatment adherence is crucial for achieving therapeutic goals. FDC combinations have the benefit of simplifying drug regimens and the advantages of its combined effects. The preference for these combinations over separate drugs is because FDC therapies with complementary mechanisms of action provide the opportunity to achieve better control with higher patient adherence and a positive safety profile [35]. The two compounds have different mechanisms of action, so the pharmacological effect is additive, which represents a benefit for these patients, where therapeutic goals are often not reached with monotherapy, requiring combination therapy.
All of this demonstrates that the atorvastatin/fenofibrate combination is safe and effective for managing mixed dyslipidemia. This finding is also consistent with reports from various international guidelines and authors regarding the management of such patients. It is worth mentioning that this combination also has the potential to slow the progression of vascular disease, reduce the risk of complications, and offer cost savings compared to using the individual components separately. Ultimately, it may also help decrease polypharmacy.
Although the present study evaluates the efficacy and safety of atorvastatin/fenofibrate, it has certain limitations. One notable limitation is the lack of analysis of specific biomarkers for assessing cardiovascular risk (ApoB, remnant cholesterol, small, dense LDL particles), which could have provided deeper insights into the clinical benefits of the investigational products. Additionally, the small sample size limits the generalizability of the findings, preventing the results from being fully extrapolated to the broader population. Finally, to assess the long-term clinical benefits, it would be valuable to conduct a follow-up over time of patients undergoing the combination therapy.

Comments (0)