
Remember me
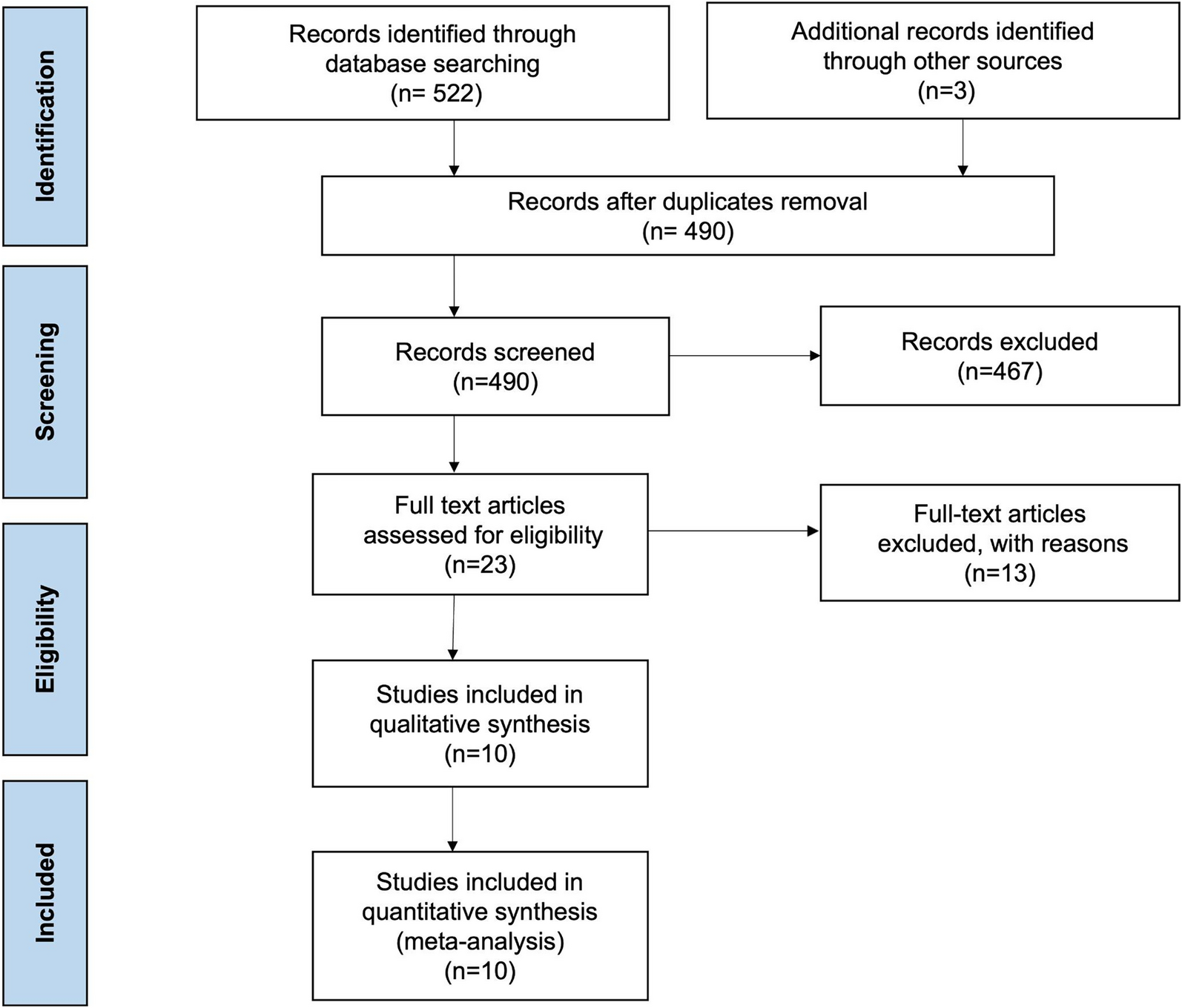
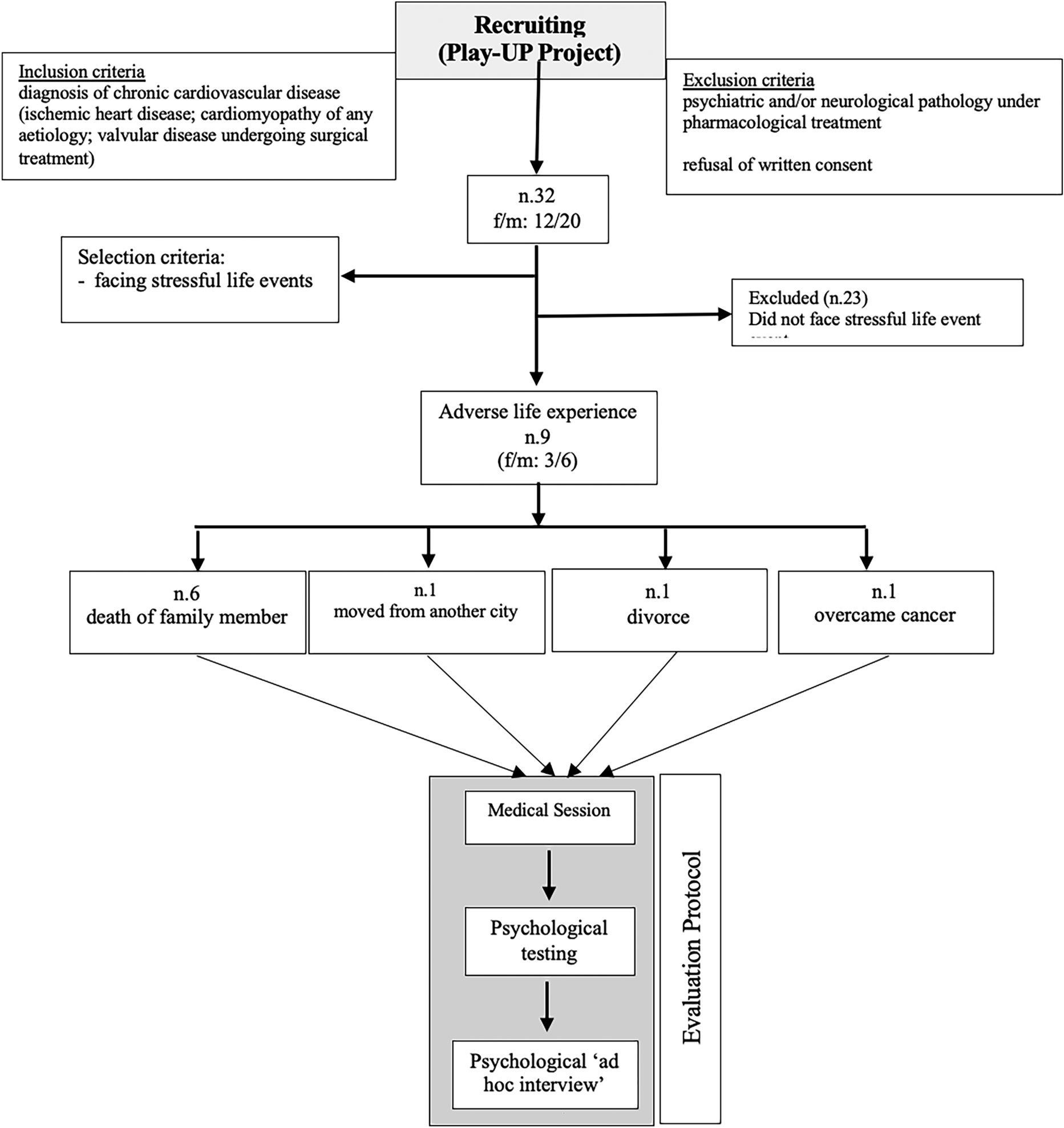
Between July 2021 and September 2022, 53 patients with ATTR-CM were enrolled in China and treated with open-label tafamidis free acid 61 mg (Fig. 1). The baseline demographics and clinical characteristics of the 53 treated patients are shown in Table 1. Mean age among all patients was 60 years, 89% were male, and 94% had ATTRv-CM. The most common TTR variant was A97S (p.A117S; in 21% of all patients). All but one patient were of Han Chinese ethnicity; all were Asian. The majority of patients (64%) had a left ventricular ejection fraction of ≥ 50%, and mild heart failure symptoms, as denoted by an NYHA functional classification of II in 81% and a NAC stage of I in 74%. Despite this, patients reported significant physical and functional limitations (mean SF-12 PCS score 28, mean 6MWT distance 290 m) and an elevated NT-proBNP concentration (mean 2950 ng/l). Patients reported fair-to-good HRQoL (mean KCCQ-OS score 58) and lower EQ-5D-5L index (mean 0.5) and EQ-VAS scores (mean 63) than might be expected for their age [13].
Fig. 1 Table 1 Baseline demographics and clinical characteristics
Table 1 Baseline demographics and clinical characteristicsAt baseline, 66% of patients took ≥ 1 cardiac medication of interest, including 38% who took a potassium-sparing diuretic, 42% another diuretic, 23% a beta-blocker, 8% an angiotensin receptor/neprilysin inhibitor, 6% an angiotensin II receptor antagonist, 4% a calcium channel blocker, 2% an angiotensin-converting enzyme inhibitor, 2% a sodium-glucose cotransporter 2 inhibitor, and 36% another cardiac therapy.
Overall, 92% of patients had an ongoing concomitant medical condition. The most frequent were hereditary neuropathic amyloidosis (17%), cardiac failure, chronic gastritis, and hypertension (each in 15%). The majority (96%) of patients took ≥ 1 concomitant medication during the study. No patient had a pacemaker fitted during the study.
Median treatment exposure among all patients was 345 (range 24–418) days, and 87% of patients received ≥ 253 days of treatment. Ten patients discontinued tafamidis treatment during the study, including six due to death and one due to a TEAE. Overall, 43 patients completed the 12 months of planned treatment.
The plasma concentration of tafamidis was evaluated in the 53 enrolled patients. Findings were consistent with those previously reported (Table S2) [18, 19].
SafetyDuring study treatment and the 28 days following the final dose, 45 (85%) patients reported ≥ 1 TEAE (129 TEAEs in total; Table 2). The nature of the TEAEs was consistent with the known safety profile of tafamidis (Table S3) [4, 6].
Table 2 Treatment-emergent adverse eventsAmong patients with TEAEs, most reported only mild- or moderate-intensity events (62% of patients with TEAEs; 105 events). There were 24 severe TEAEs reported in 17 patients; those reported in > 1 patient were cardiac failure (n = 6); COVID-19 infection (n = 3); and acute cardiac failure, disease progression, and pneumonia (n = 2 each). A total of 31 SAEs were reported in 47% of patients with TEAEs (Table S4); the most common were cardiac failure (n = 6); acute cardiac failure and COVID-19 infection (n = 3 each); disease progression and pneumonia (n = 2 each). One patient discontinued the study due to a TEAE of hemorrhagic cerebral infarction that was not considered to be treatment-related. Three patients each reported one TEAE that was considered to be treatment-related: abnormal hepatic function (mild severity), gouty arthritis (moderate severity), and hematuria (mild severity). Of these, one patient (with the TEAE of gouty arthritis) had a temporary dosing amendment.
There were six deaths reported; none were considered related to treatment: two were due to disease progression; two due to aggravated heart failure; one due to syncope; and one due to COVID-19 infection, severe pneumonia, and respiratory failure.
EfficacyAfter 6 and 12 months of treatment with tafamidis, there were minimal changes from baseline in all efficacy measures, suggesting stabilization of ATTR-CM progression (Fig. 2). At month 12, mean change from baseline in 6MWT distance was 2 m, NT-proBNP concentration − 422 ng/l, troponin I concentration 0 µg/l, KCCQ-OS score − 0.3, SF-12 PCS score 0, SF-12 MCS score 1.5, EQ-5D-5L index score 0, and EQ-VAS score 3. Additionally, mean (SD) change from baseline in eGFR was − 1 ml/min/1.73 m2 (20.4; n = 48) at month 6 and − 4 ml/min/1.73 m2 (22.8; n = 41) at month 12.
Fig. 2
Change in efficacy measures at 6 and 12 months. 6MWT 6-min walk test, EQ-5D-5L 5-level EQ-5D, EQ-VAS EQ visual analog scale, KCCQ-OS Kansas City Cardiomyopathy Questionnaire Overall Summary, MCS Mental Component Summary, NT-proBNP N-terminal pro-B-type natriuretic peptide, PCS Physical Component Summary, SD standard deviation, SF-12 12-item Short Form Survey
Using clinically relevant thresholds to define deterioration, exploratory analyses showed substantial proportions of patients experienced stability or improvement in each disease measure at months 6 and 12 (Fig. 3). At month 12, 65% of patients showed stability or improvement in 6MWT distance, 95% in NYHA class, 93% in NAC stage, 70% in NT-proBNP concentration, 45% in troponin I concentration, 65% in KCCQ-OS score, 53% in EQ-5D-5L index score, and 77% in EQ-VAS score.
Fig. 3
Proportion of patients with stability or improvement in efficacy measures. 6MWT 6-min walk test, EQ-5D-5L 5-level EQ-5D, EQ-VAS EQ visual analog scale, KCCQ-OS Kansas City Cardiomyopathy Questionnaire Overall Summary, NAC National Amyloidosis Centre, NT-proBNP N-terminal pro-B-type natriuretic peptide, NYHA New York Heart Association
Comments (0)