
Remember me
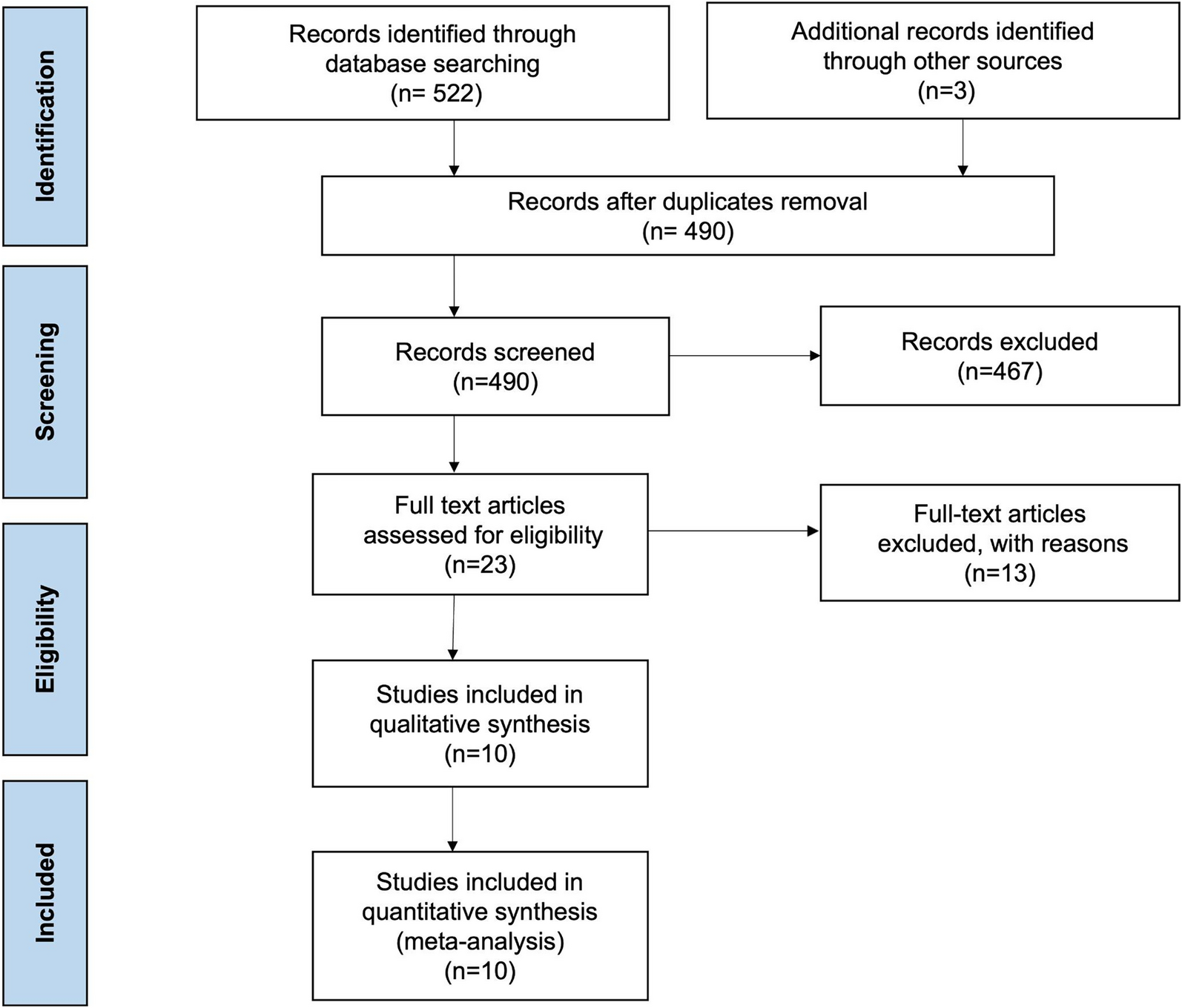
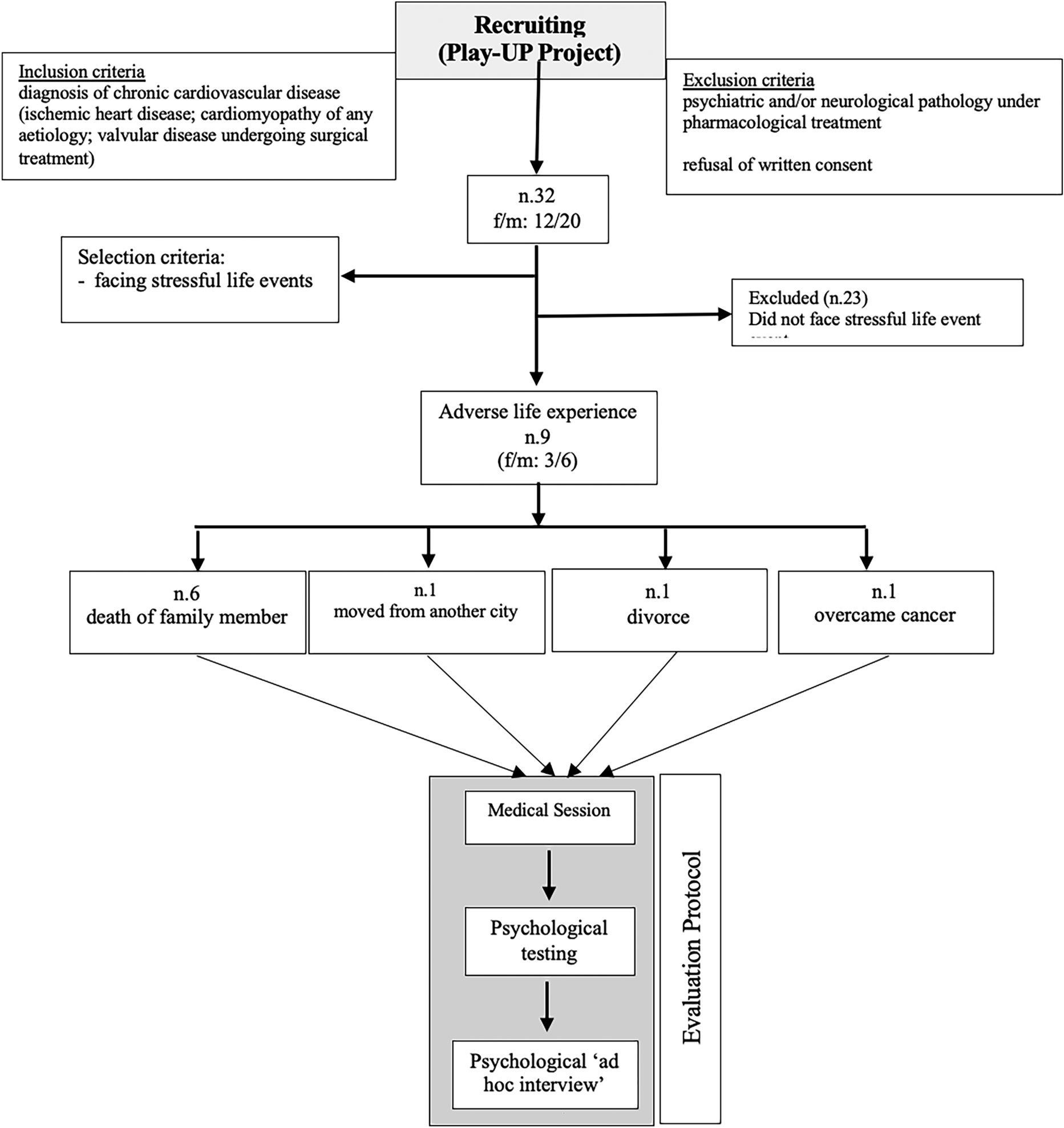
This retrospective, observational, single-center study was conducted at Shanghai Ninth People’s Hospital Affiliated with the Shanghai Jiaotong University School of Medicine from January 2022 to December 2023. A total of 191 patients with nonvalvular AF were initially enrolled in the study, all of whom had undergone successful LAAC treatment without procedure-related complications and peri-device leakage (PDL). All of these patients met the following inclusion criteria: age > 18 years; CHA2DS2-VASc score ≥ 2; and at least one of the following conditions: high bleeding risk (HAS-BLED score ≥ 3); history of stroke or systemic embolism despite OAC therapy; or refusal to take OAC. Subsequently, four patients were excluded from participation due to DRT and 14 were excluded due to PDL at 3 or 6 months after the LAAC procedure, as assessed using TEE or CCTA. Ultimately, 168 patients were eligible for inclusion in the analysis in the present study (Fig. 1).
Written informed consent was obtained from all participants prior to the procedure. All patients were informed of the purpose of the study, the use of their clinical and imaging data for research purposes, and their right to withdraw at any time without their medical care being affected. This research complied with the Declaration of Helsinki guidelines and was approved by the Ethics Committee of Shanghai Ninth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (Ethical Approval number: SH9H-2024-T142-1).
Fig. 1
Timeline of study design and patient selection
Procedure and Medical TreatmentPrior to the LAAC procedure, CCTA and TEE images were routinely acquired to exclude LA or LAA thrombus and to measure the dimension of LAA in order to ensure its compatibility with the implantation of a closure device. LAAC was performed under general anesthesia with TEE and fluoroscopy guidance. LAAC devices used in the present study included Watchman™ (Boston Scientific, Marlborough, MA, USA) and LACBES™ (Pushi Medical Device Corp, Shanghai, China) devices. Clinical and imaging data were retrospectively collected from the electronic medical records by trained research staff who were blinded to IDE status. All device implantations were carried out in accordance with established criteria, namely, the Position-Anchoring-Size-Seal (PASS) principle for the Watchman device and the Proper Position-Absolute Anchor-Separate Seal-Typical Tire (PAST) guideline for the LACBES device. Following the procedure, all patients were placed on OAC therapy during the initial follow-up period.
All patients received antithrombotic treatments in the initial 3 months post-procedure, including OACs for patients with Watchman devices and either OACs or dual antiplatelet therapy (DAPT) for those with the LACBES occluder. At the 3-month follow-up, patients without evidence of DRT were transitioned from anticoagulation to dual antiplatelet therapy, consisting of daily aspirin (100 mg) and clopidogrel (75 mg), which was continued up to 6 months post-implantation.
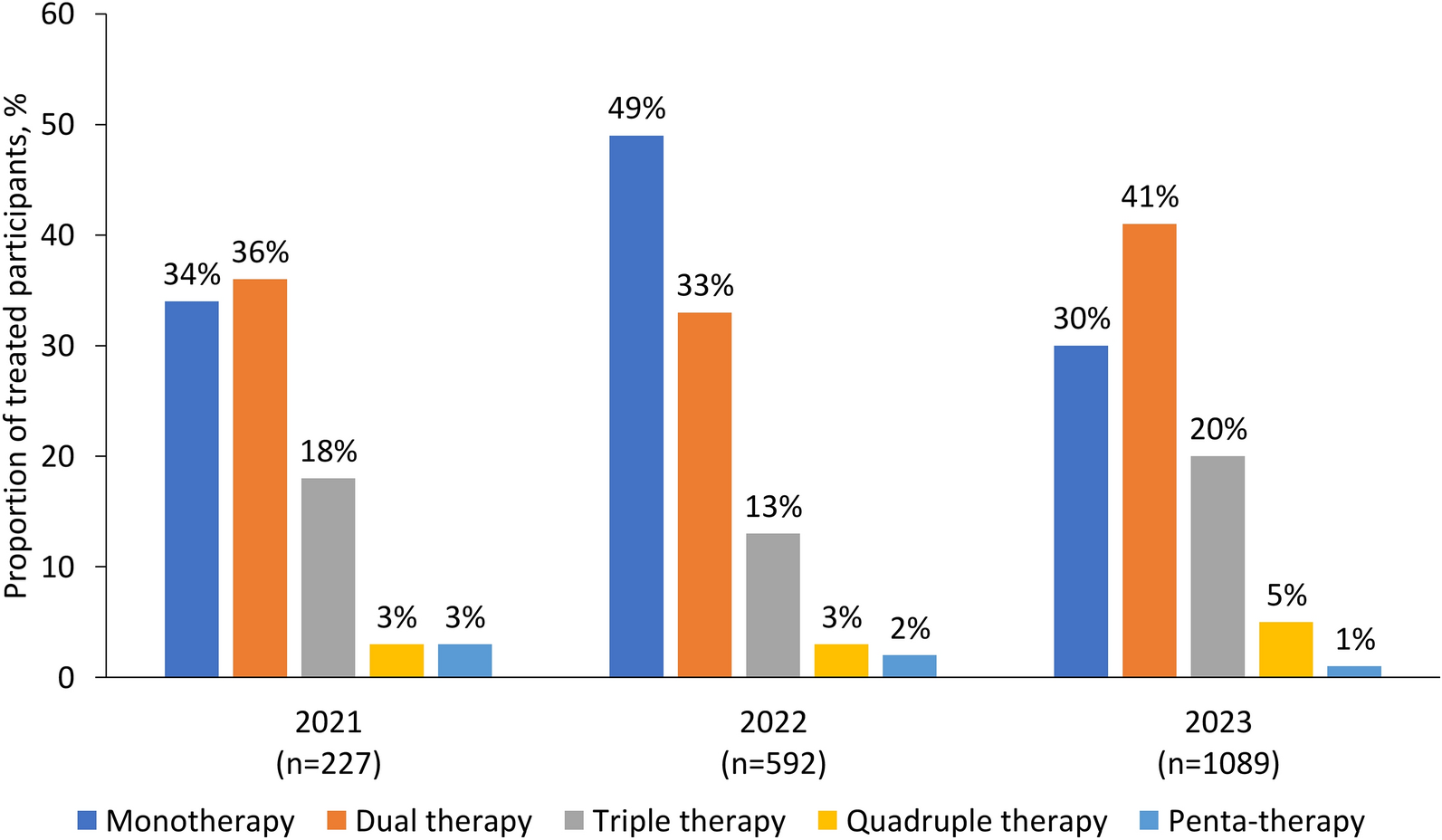
DefinitionsSuccessful LAA closure in the present study was defined as the absence of PDL during the procedure, as confirmed by both TEE and angiography. At the 6-month follow-up, TEE was used to assess for the presence of PDL, defined as color Doppler–detected peri-device flow, and for DRT, defined as thrombus attached to the luminal surface of the occluder. In contrast, IDE was assessed exclusively using CCTA. IDE was defined as either a LAA attenuation > 100 Hounsfield units (HU), an LAA-to-left atrium attenuation ratio ≥ 0.25, or as evidence of trans-fabric leak, as previously described in published criteria [19, 20] (Fig. 2).
Fig. 2
Imaging characteristics of complete and incomplete endothelialization as assessed by cardiac computed tomography angiography (CCTA) and two-dimensional transesophageal echocardiography (TEE). Red arrows indicate leakage of contrast into the left atrial appendage
Indexes for IR were calculated as follows:
TyG = Ln [TG (mg/dL) × FPG (mg/dL)/2], where FPG is fasting plasma glucose;
TG/HDL-c = TG (mg/dL) ÷ HDL-c (mg/dL);
METs-IR = Ln [(2 × FBG (mg/dL)) + TG (mg/dL)] × BMI (kg/m2))/(Ln [HDL-c (mg/dL)]), where FBG is fasting blood glucose and BMI is the body mass index.
.
Cardiac CT ImagingThe CCTA protocol has been described previously [21]. Cardiac computed tomography (CT) with electrocardiograph (ECG) gating was conducted using a dual-source 64-slice SOMATOM Definition Flash scanner (Siemens, Forchheim, Germany), capturing both arterial and venous phases. The scanning protocol utilized a temporal resolution of 330 ms and detector collimation of 64 × 0.6 mm. Each patient received 50–70 mL of iodinated contrast agent (Iohexol, 350 mg iodine/mL) administered at 5.0 mL/s. Post-processing and image interpretation were performed using the Extended Brilliance Workspace version 4.5 (Philips Healthcare, Best, The Netherlands), and all scans were independently reviewed by two experienced radiologists blinded to clinical data.
TEE ImagingBoth two (2D)- and three-dimensional (3D) TEE were performed with a Philips Healthcare Epiq7C ultrasound machine for cardiovascular imaging. According to standard guidelines, LAA images were obtained at 0°, 45°, 90°, and 135° at the mid-esophageal level. Doppler imaging of the PDL in each view was performed at 3 or 6 months after the LAAC procedure by an echocardiographer who was trained in follow-up and blinded to the procedural information and CCTA results.
Statistical AnalysisContinuous variables were analyzed for a normal distribution using the Shapiro–Wilk test, and presented as the mean ± standard deviation (SD) or the median with interquartile range. The independent t-test or Mann–Whitney U-test was used to compare data between two groups. All clinical and laboratory variables were initially subjected to univariate logistic regression analysis to identify potential predictors of IDE. Variables with p-values < 0.05 in the univariate analysis were included in the multivariate logistic regression model using a forward stepwise selection approach. Multicollinearity was assessed using the variance inflation factor (VIF), and all included variables had VIF values < 4, indicating no significant collinearity.
Categorical variables were assessed using Fisher’s exact test or the chi-square test. Statistical analysis was performed with SPSS version 20.0 software (SPSS IBM Corp., Armonk, NY, USA). A receiver operating characteristic (ROC) curve was used to evaluate the validity and the boundary value was calculated. A two-sided p-value of < 0.05 was considered to indicate statistical significance.
Comments (0)