
Remember me

We used the EUROmediCAT central database, a European research consortium dedicated to improve drug safety in pregnancy [34]. This database includes all live births, fetal deaths at 20 weeks of gestation or later, and terminations of pregnancy for fetal anomalies (TOPFA) with congenital anomalies at any gestational age. In July 2024, this database included 25 congenital anomaly registries in 17 European countries, covering more than 13 million births.
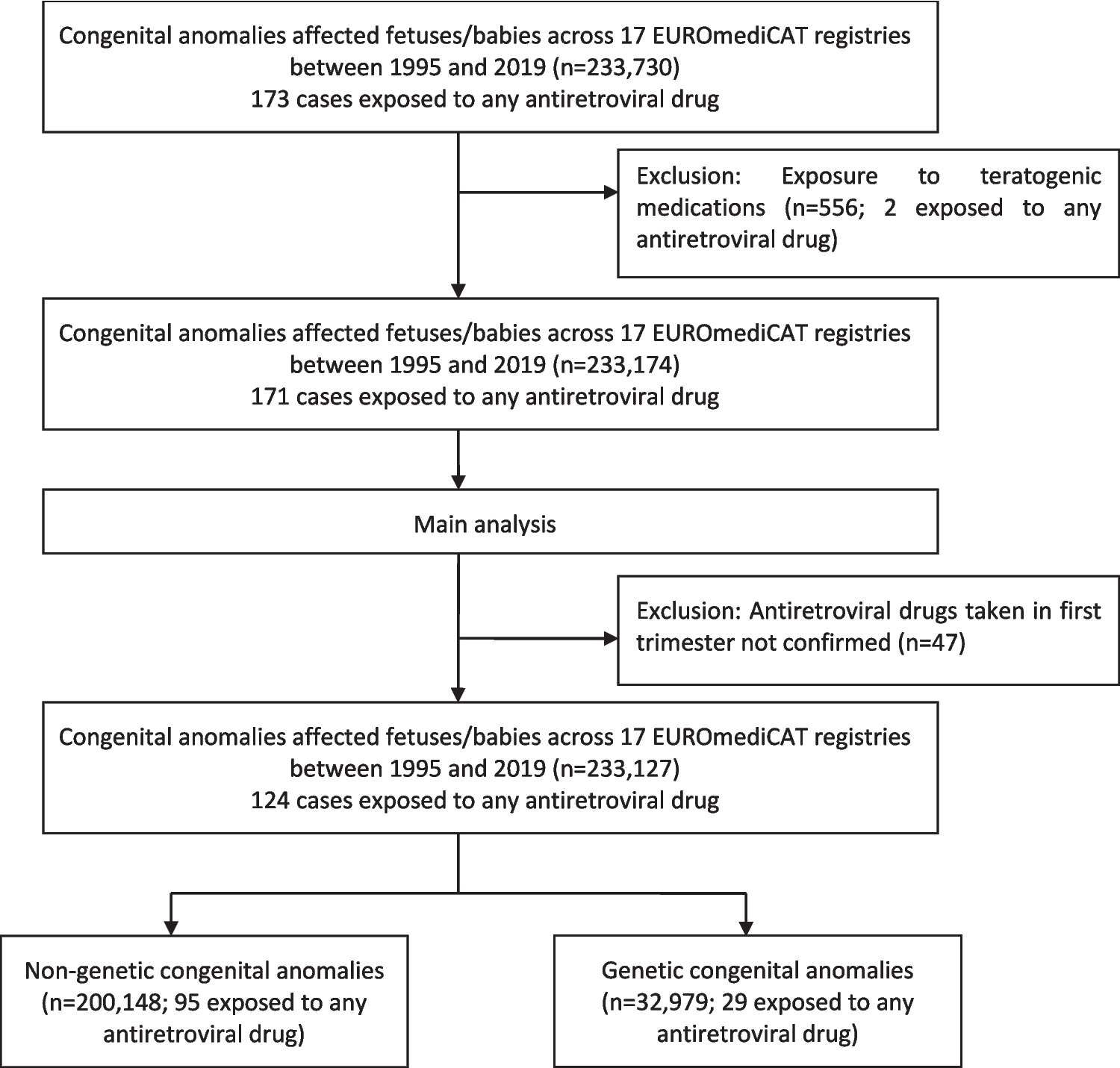
The data provided anonymized information about the registry (center number, location), the mother (age, family history, disease diagnosed before or during pregnancy), the maternal drug exposure (drugs received during pregnancy and drugs received especially in the first trimester of pregnancy), and the baby (singleton or multiple births, gestational age at birth/termination, birth/termination year, sex, birth weight, syndromes, and congenital anomalies, age at diagnosis of congenital anomalies). All the data were collected as described in the EUROCAT Guide 1.4, the applicable guide at the time of analysis [35]. The congenital anomalies were coded according to the International Classification of Diseases ICD9 (740–759) and ICD10 (Q00-Q99) with British Pediatric Association (BPA) extension and classified into subgroups according to the EUROCAT classification. Registrations with minor congenital anomalies only according to the EUROCAT definition were excluded. Therefore, only major congenital anomalies were selected in this study. All registries participating in EUROmediCAT, which have given the approval to share and investigate data (n = 17), were included. The selection of the study population is summarized in Fig. 1.
Fig. 1
Flowchart of the study population selection in the main analyses of congenital anomalies observed in birth outcomes exposed to any antiretroviral drug from the first trimester of pregnancy in the EUROmediCAT central database between 1995 and 2019
Study designWe conducted a case/non-case study [36,37,38,39] to investigate the effect of exposure to antiretroviral drugs in the first trimester of pregnancy and the occurrence of congenital anomalies, using the EUROmediCAT central database from 1995 to 2019, according to data availability at the time of study analysis as of October 2023. A signal verification analysis to investigate associations previously reported in the literature, and then a signal detection analysis to identify potential new signals between exposure to any antiretroviral drugs and specific congenital anomalies were performed.
Study populationIn this study, we included all the congenital anomalies reported in live births, fetal deaths after 20 weeks of gestation, or TOPFA, exposed to any antiretroviral drugs, from January 1, 1995, to December 31, 2019, declared in the EUROmediCAT database. Importantly, the databases do not include any data on babies/fetuses without a congenital anomaly. Consequently, we conducted a case/non-case study using malformed controls, comparing antiretroviral exposure among registrants with a specific congenital anomaly with antiretroviral exposure among all other registrants.
Case-malformed/case-controlled definition and exposure definitionExposed cases/non-cases with co-medications with known teratogenic effects were excluded (additional file number 1). First, for the signal verification analysis, we defined cases as all live births, fetal deaths from 20 weeks gestational age, and TOPFA with major congenital anomaly (classified by EUROCAT subgroup) which were signals identified from the literature for specific antiretroviral drug exposures, excluding those with a genetic syndrome. Non-cases were all other registrants. Second, for the signal detection analysis, all major congenital anomalies categorized by organ system were defined in turn as cases. All EUROCAT anomaly subgroups were analyzed as cases, with a changing control group consisting of all other registrants. We compared a specific congenital anomaly (“case group”) to other registrants with a diagnosis of a major congenital anomaly after the exclusion of the specific congenital anomaly being analyzed (“non-case control group”). For specific congenital anomalies, such as neural tube defects or hypospadias, we excluded other congenital anomalies in the same organ system category from the control group. Moreover, only male fetuses/babies were included in the analysis of hypospadias risk. The unexposed groups were defined for registrants without the use of any antiretroviral drugs. The control groups were classified into two categories according to the EUROCAT definition of a genetic condition (Guide 1.4): one that excluded genetic and chromosomic anomalies and one that included all non-genetic and non-chromosomal cases.
Exposure to antiretroviral drugs during the first trimester of pregnancy was defined according to the EUROCAT guide 1.4 [35] as the period from the first day of the last menstrual period to 12 completed weeks of gestation (day 0 to day 83). Antiretroviral drugs were coded according to the Anatomical Therapeutic Chemical (ATC) codes (J05A-E/F/G/R/X), reported by the World Health Organization (WHO). As the exposure period was not available for some cases included in the EUROmediCAT database, we conducted statistical analysis only in congenital anomaly cases for which maternal exposure during the first trimester was confirmed. All cases (with maternal exposure during the first trimester confirmed or not) were evaluated in a sensitivity analysis.
Identification of congenital anomalies reported in the literatureA literature review was conducted to identify the previous congenital anomaly signals observed after exposure to antiretroviral drugs and guide our data analysis of the EUROmediCAT central database. Bibliographic searches were conducted from PubMed, Web of Science, Embase, Cochrane Library, and Reprotox. To be included, cohort studies had to have been conducted between 1995 and 2019, in high-income countries, in HIV-positive pregnant women exposed to antiretroviral drugs, in order to provide representative studies designed on data collected in the EUROmediCAT database. The inclusion criteria were similar to those applied for the population included in the EUROmediCAT central database: all congenital anomalies and all antiretroviral drugs (defined from the ATC code) were eligible.
Data analysisFirst, for all major congenital anomaly cases exposed to antiretroviral drugs, we described the distribution by registry data, maternal data (age, diseases before and during pregnancy, exposure to antiretroviral drugs), and birth data (singleton or multiple births, gestational age at birth, sex, birth weight, age at diagnosis of congenital anomalies, congenital anomalies classified by organ system). Quantitative variables were reported as mean with standard deviation, and categorical qualitative variables as numbers with percentages. Second, we conducted a signal verification study for each signal between exposure to antiretroviral drugs and a subgroup of congenital anomalies identified in the literature. Third, if less than 15 cases were exposed to a specific antiretroviral drug, an accurate description of each case, including associated genetic diagnosis, was provided (additional file number 2). Last, if there are more than 15 exposed cases of the same antiretroviral drug and more than three similar birth defects, we then conducted a signal detection analysis to detect any potential new signals.
In the signal verification study and the signal detection study, when an ATC code could not allow to identify specific antiretroviral drugs, we included these cases only in the descriptive analysis. Then, we conducted a disproportionality analysis [36,37,38,39] to estimate the reporting odds ratio (ROR) and their 95% confidence intervals (95% CI), comparing the odds of exposure in registrants with specific non-genetic congenital subgroups of anomalies (cases) to the odds of exposure among registrants with another non-genetic or genetic congenital anomalies (non-case controls), using logistic regression models. For these analyses, each antiretroviral drug was evaluated separately, the other antiretroviral drugs being excluded from the unexposed comparison group (cases and non-cases). ROR was estimated for each subgroup of congenital anomalies, defined according to the EUROCAT classification. The main analyses were performed only in congenital anomaly cases for which maternal exposure during the first trimester was confirmed. All cases (with maternal exposure during the first trimester confirmed or not) were evaluated in a sensitivity analysis. In the signal verification analysis, ROR was adjusted in logistic regression models for registry and maternal age (five categories: 14–19, 20–29, 30–40, ≥ 41 years), and we defined a significant signal of disproportionality when the lower limit of the 95% CI of the ROR was higher than one [40]. We performed a complete case analysis, namely, registrants with missing data for any of the adjustment covariates were excluded from the multivariable analyses. For the signal detection analyses, we corrected the p-values with the Bonferroni rule to take into account the issue of multiple testing; hence, we considered a signal to be significant if the p-value was below 0.0015 (as 33 comparative tests were made). Finally, when a signal was highlighted in signal detection analyses for a specific antiretroviral drug, we conducted statistical analyses for the most frequent combinations of antiretrovirals (example: tenofovir/emtricitabine). Statistical analyses were performed on Statistical Analysis Software (SAS® version 9.4).
Comments (0)