
Remember me

This study was a sub-analysis of the “Low-dose colchicine for secondary prevention of cardiovascular disease 2” (LoDoCo2) trial, which was a randomized, double-blind, placebo-controlled study conducted in the Netherlands and Australia from 2014 to 2019. In short, this cardiovascular outcomes trial investigated efficacy of 0.5 mg colchicine daily in patients with chronic coronary syndrome. The design and outcomes of the study have been published elsewhere [3, 14].
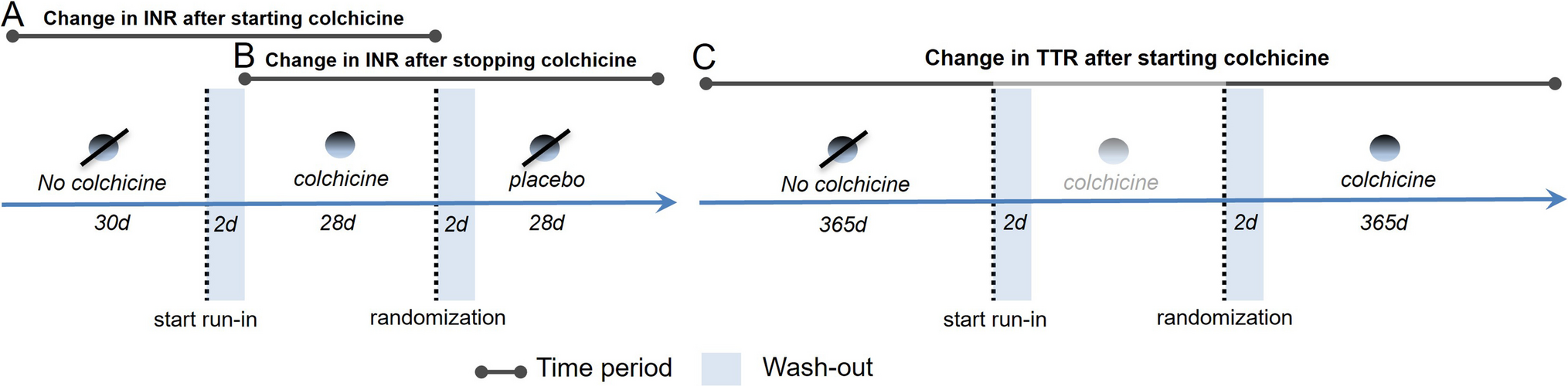
This sub-analysis included all VKA users from the LoDoCo2 study at three Dutch hospitals: Meander Medical Center (MMC), Northwest Hospital Group (NWG), and Isala Meppel (IM). Patients were treated with acenocoumarol or phenprocoumon, as warfarin is not prescribed in the Netherlands. These large, representative institutions had readily accessible international normalized ratio (INR) measurements. Patients were included if they were treated with VKA and had at least six INR measurements available prior to study participation to ensure continuous use. The INR and VKA dosage data were collected as part of routine care and obtained from the thrombosis services at the participating hospitals. The timeline of the LoDoCo2 and the current study is depicted in Fig. 1. Eligible patients entered an open-label run-in phase for 30 days, in which they received 0.5 mg of colchicine once daily, followed by randomized allocation to either continue with colchicine or switch to placebo. The follow-up period for patients extended from 1 year prior to the study until 1 year after randomization.
Fig. 1
Research timeline overview VKA vitamin-K antagonist, INR international normalized ratio
OutcomesThe primary outcome of the sub-study was the intra-patient difference in INR during the first month after starting or stopping colchicine as compared to the preceding month. Change in INR was measured after the introduction of open-label colchicine during the run-in phase (a pre-post comparison of no colchicine versus colchicine) and change in INR after the introduction of placebo during the randomized phase of the trial (a pre-post comparison of colchicine versus no colchicine). To minimize potential interference from the thrombosis service and accurately assess the potential drug-drug interaction between colchicine and VKAs on INR, an intra-patient comparison approach was used. This was assessed in two phases: (A) after the start of colchicine treatment during the open-label run-in phase (Fig. 1A) and (B) directly after switching to placebo, reflecting the discontinuation of colchicine (Fig. 1B). During these treatment switches, the first INR measurement in the new period was compared to the most recent INR measurement in the preceding time window, allowing a washout of 2 days (i.e., the first 2 days after switching treatment regimen were excluded from the analysis) and minimizing interference from the thrombosis services.
Secondarily, in a similar manner, intra-patient difference in VKA-dosage was compared between the previously defined time windows (Fig. 1).
Finally, to investigate the long-term impact of colchicine on VKA efficacy, time in therapeutic range (TTR) was assessed by comparing each patient’s TTR in the 365 days after randomization with their TTR in the equivalent period before trial participation (Fig. 1C). The TTR was determined using the Rosendaal method, which utilizes linear interpolation to estimate the actual days spent within the therapeutic range [15]. A therapeutic INR was defined as 2.0–3.0 or 2.5–3.5, depending on the indication.
The occurrence of extreme INR values, defined as INR values > 5.0 or < 2.0, was also examined during the 30 days before and after initiating colchicine therapy.
Collected co-variables included age (continuous), sex, VKA type (acenocoumarol and phenprocoumon), VKA indication (atrial fibrillation, mechanical heart valve, pulmonary embolism, venous thromboembolism, thrombus in the heart, stent, cardiomyopathy, and aneurysm), and interacting drugs (i.e., those enhancing or inhibiting the effect of VKAs). The latter were selected from the Medical Pharmaceutical Decision Rules from The Royal Dutch Pharmacists Association KNMP-MFB, Micromedex interaction checker, and the Federation of Dutch Thrombosis Services (FNT). Included drugs are stated in the footnote of Table 1.
Table 1 Baseline characteristics of patientsAnalysisNo reliable in vivo estimates of the expected change in INR after introducing colchicine are available in the literature. We aimed for an INR positioned centrally within the therapeutic range—2.5 for low- and 3.0 for high-intensity therapy. Given that a shift of 0.5 in INR would place values outside this target range, we considered this change clinically significant. To detect an INR difference of 0.5, using α = 0.05 and β = 0.20, a sample size of at least 20 would be required. We deliberately chose this difference in mean INR to capture potential drug-drug interactions effectively.
Continuous variables are presented as means or medians with standard deviations and interquartile ranges for normally and non-normally distributed variables, respectively. Distributions were assessed using the Kolmogorov–Smirnov test, in addition to visual inspection with Q-Q plots and histograms. Categorical variables were presented as counts and percentages.
Intra-patient changes in INR, VKA dosage, and TTR were analyzed using paired T-tests with a two-sided significance level of 0.05. The data were stratified by sex, VKA type, age, and the total number of interacting medications each patient was using.
All data handling and statistical analyses were conducted using SAS 9.4.
This study involved a re-analysis of data, with additional data obtained from the Dutch Thrombosis Services. The re-analysis fell under previous medical ethics approval and was conducted in compliance with existing approvals ACTRN12614000093684.
Comments (0)