Participants and study design
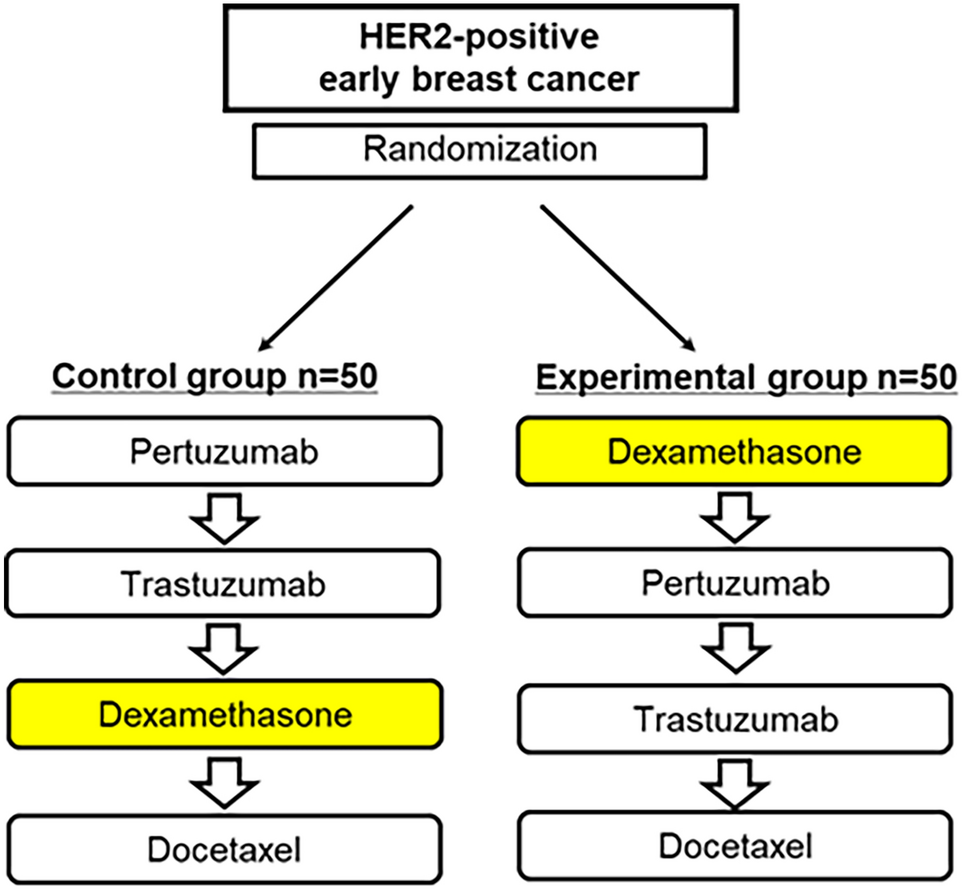
This is a prospective, multicenter cohort study. None of the consulted ethics committees raised concerns regarding its conduct, and the study was registered in the German Clinical Trials Register on 6 May 2019 (DRKS00016761). Participants in this study were female patients with histologically confirmed early breast cancer, i.e., Union for International Cancer Control (UICC) stages I–III, excluding patients with no tumor (T0), with a carcinoma in situ (Tis) or with a microinvasion (T1mic), and scheduled to receive neoadjuvant chemotherapy according to guidelines [4]. Participants had an Eastern Cooperative Oncology Group (ECOG) performance score of 0–2, an age between 18 and 80 years, no current pregnancy, no concomitant medication critically influencing their ability to follow the requirements of the clinical observation, no participation in a clinical trial or use of an investigational agent from four weeks before the first until the last chemotherapy cycle, and had given signed informed consent. Participants were treated in four certified breast cancer centers, two in Southern and Eastern Germany each, in one large- and one medium-sized city in each region (Munich, Berlin, Esslingen, Brandenburg a. d. Havel).
The observation started with participant inclusion, before the first cycle of neoadjuvant chemotherapy, and ended 2 weeks after surgery or, if surgery was not performed, 2 weeks after the last chemotherapy cycle, in order to measure the effect of the last treatment step after a time interval comparable to the previous steps. In addition to data from patient records, standardized questionnaires were filled out by the patients.
All collected data were transferred into the clinical data management system Marvin EDC (XClinical GmbH, Munich, Germany) using electronic case report forms (eCRFs) developed by the Gesellschaft für klinische Forschung e.V. (GKF). Permanent centralized monitoring was performed together with on-site-monitoring in each center 8 weeks after inclusion of the first participant and thereafter on a risk-based approach to ensure patient safety, data completeness and accuracy. Data managers of the GKF checked the eCRF database for new entries on a daily basis. Conspicuous data (e.g., missing data, data outside reference ranges) were flagged as query within the eCRF system, eliciting a request for check by the data-entry study personnel. A patient's eCRF documentation could not be electronically signed and locked if queries were still unresolved. At the end of documentation and data cleaning the data were transferred into SAS data formats and analyzed with SAS for Windows version 9.4 (SAS Institute Inc., Cary, NC, USA).
Demography, tumor factors and chemotherapy regimens
Demographic and tumor factors were collected at the qualifying examination including age, menopausal status, tumor stage, nodal stage, tumor grading, Ki-67 score, estrogen-receptor (ER) status, progesterone-receptor (PR) status, human epidermal growth factor receptor-2 (HER-2) status, ECOG-score, BMI and concomitant diseases.
Recording of chemotherapy drugs and regimens started with the first chemotherapy cycle, which defined the baseline visit. Thereafter, visits during the whole observation time were documented every 2 or 3 weeks, depending on the density of the anthracycline cycle, i.e., whether it was given every 2 (dose-dense) or 3 weeks (standard).
Patient-reported quality of life and symptoms assessment
Primary outcomes of this study were ‘general fatigue’, as assessed by the Multidimensional Fatigue Inventory (MFI), and HRQoL as assessed by the Trial Outcome Index (TOI) of the Functional Assessment of Cancer Therapies – Breast Cancer (FACT-B). The MFI is a self-report instrument designed to measure fatigue. It consists of 20 items grouped in five dimensions: general fatigue, physical fatigue, mental fatigue, reduced motivation and reduced activity. Patients indicate on a 1- to 5-point scale to what extent the corresponding statement applies to them. One score between 4 and 20 is generated per dimension. The higher the score, the higher the fatigue perceived by the patient [18]. The FACT-B is a self-report instrument designed to measure multidimensional HRQoL in patients with breast cancer. In its fourth version, it consists of 37 items with five ordered categorical answers. FACT-B items are grouped into the subscales physical, social, emotional and functional well-being, with score ranges of 0–28, 28, 24, 28, respectively, and an additional breast cancer subscale with a score range of 0–40. The TOI summarizes the physical, the functional well-being and the breast cancer subscales with a score range of 0 to 96. The FACT-B total score summarizes all subscales with a score range of 0 to 148. The higher the score, the better is the HRQoL [19]. The MFI and FACT-B were completed by participants before chemotherapy at visits defined by the protocol, i.e., every 2 or 3 weeks (see above).
Secondary outcomes of this study were the incidence and severity of adverse events arising during neoadjuvant chemotherapy. The severity of adverse events was documented according to the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0. Adverse events were classified according to the Medical Dictionary for Regulatory Activities (MedDRA), version 22.1, by data managers of the GKF.
Statistical analyses
While no confirmatory interpretation of statistical results was intended, the planned sample size of 50 patients was chosen for having a power of 80% to detect a standardized mean difference of 0.4 for the change from baseline to the end of the study in one of the primary efficacy parameters. All analyses of the primary and secondary outcomes were done with the Full Analysis Set which included all patients fulfilling the inclusion/exclusion criteria, having given informed consent and having at least one follow-up after the baseline visit. There was only one patient who dropped out of the study immediately after the qualifying examination and for whom no further efficacy- or safety-relevant data were documented.
Demographic and baseline characteristics, as well as outcome parameters, are presented by descriptive statistics, including median and interquartile range (IQR) in case of quantitative data, and contingency tables showing absolute and relative frequencies for categorical data. Results of statistical tests are shown as estimates, 95% confidence intervals and corresponding p-values, which were interpreted in exploratory intent only, which is why no adjustment for multiple testing was done. As an exception, in accordance with good statistical practice, the p values of the two primary outcome parameters were evaluated after Bonferroni-Holm adjustment for multiple testing, with statistical significance claimed only when the smaller p value was less than half the global α error level, i.e., 2.5%.
Missing data were considered in general as 'missing at random', which is reasonable since only five out of 54 included patients (9.3%) terminated chemotherapy early, one directly lost to follow-up after qualifying examination, the other four after 14 to 21 weeks of chemotherapy. Missing data were not substituted, with two exceptions. First, missing individual items of the MFI and FACT-B questionnaires were supplemented according to the respective guidelines. Second, MFI and FACT-B baseline scores still missing after this supplementing procedure were estimated by linear regression based on all available data, with patients and patient*time interactions included as fixed factors in the model.
The MFI and FACT-B results of all Full Analysis Set patients were analyzed by a linear covariance pattern model which included the respective baseline values and baseline*time interactions as independent covariates. In addition, the model contained the density of anthracycline cycles (standard vs. dose-dense), the time since start of chemotherapy, and their interaction as fixed factor and covariate, respectively. Dependent parameters were the change from baseline of the specific dimensions of the MFI or FACT-B, respectively. Of these, the MFI general fatigue scale and the FACT-B TOI represented the primary efficacy parameters of the study, while other MFI dimensions and FACT-B subscales were regarded as the secondary parameters. To account for dependencies between intra-individual measurements, a first-order autoregressive covariance structure between adjacent time points was chosen. Since most chemotherapy regimens consisted of two drug combinations, epirubicin with or without cyclophosphamide (Epi ± Cyc) and (nab-)paclitaxel with or without carboplatin (Pac ± Car), administered in this or reverse order, in a subsequent analysis of these regimens we additionally included the type and order of these drugs in the statistical model together with their respective interactions with the duration of their administration. Density of chemotherapy cycles was removed from this model, since this factor was found to be uninformative in this parameter constellation.
In sensitivity analyses of the primary statistical model, possible confounders (age, BMI, UICC stage) were added to the original model in a multivariate variable selection procedure to estimate their impact on primary outcome parameters.
Analysis of adverse events focused on patients receiving Epi ± Cyc and Pac ± Car due to the small number of patients (N = 3) and adverse events under other drug combinations. Adverse events were evaluated according to their MedDRA classification, severity and prevalence during treatment. Adverse events were also classified into “new onset” and “ongoing” adverse events and were analyzed separately. “New onset” describes adverse events documented for the first time in the patient’s observation time. “Ongoing” adverse events have already been documented for this patient during the previous drug combination. Incidences of AEs of severity grade ≥ 2 between the drug combinations were estimated separately for each diagnose using exact logistic regression. No order or interaction term was considered in this specific model for the sake of model stability. Yet, for 'new onset' adverse events, the model additionally included the individual patients as strata to account for within-patient dependencies. Over all AEs, hazard rates (HR; number of adverse events per week per patient) were calculated using a Poisson regression model including the drug combination as fixed factor and the (logarithmized) duration of the respective combination’s treatment time as offset parameter to account for different drug treatment durations. For 'new onset' adverse events, the order of the respective drug combination and order*drug combination interaction were also added to the model, as well as a random factor controlling for the dependencies between intra-individual measurements of consecutive sequences. Finally, reasons for premature chemotherapy termination were listed in the supplementary data.

Comments (0)