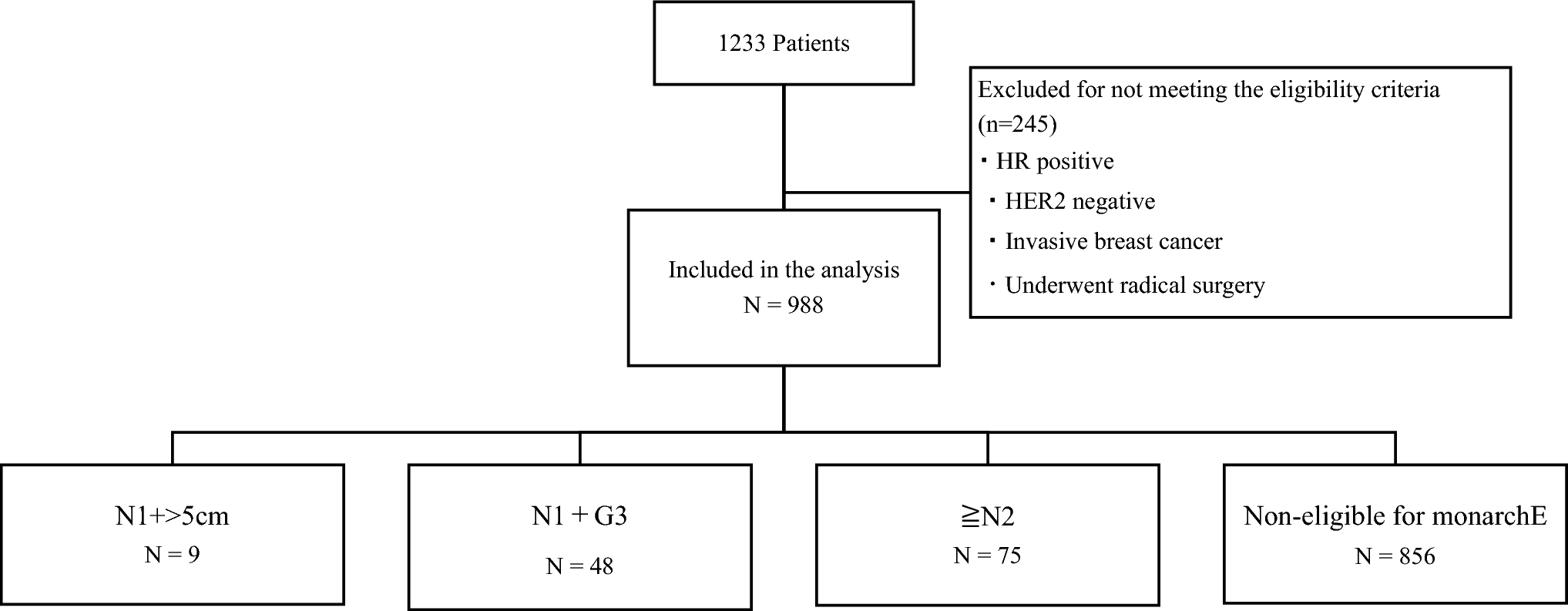
Risk stratification has become increasingly important in tailoring adjuvant therapy for HR-positive, HER2-negative breast cancer. Notably, when correlated with the 8th edition of the American Joint Committee on Cancer (AJCC), the staging of the three groups of MonarchE Cohort 1 differed [13]. According to the 8th edition of the AJCC pathological staging system, the three monarchE Cohort 1 subgroups correspond to distinct stages: the N1 + >5 cm group mainly aligns with stage IIB–IIIA, the N1 + G3 group spans stages IIA–IIIA, and the ≥N2 group includes more advanced stages such as IIIA–IIIC. These differences in staging further reflect the heterogeneity in baseline prognosis, supporting the need for more individualized risk profiling beyond eligibility criteria alone.
Patients with N2 present with higher stages, which is consistent with the increased risk observed in this group. The N1 + >5 cm subgroup is presumed to include slightly lower-risk cases, such as Stage IIB, which may explain the lack of a significant difference in iDFS in the multivariate analysis than the NAC group. Our finding that NAC independently predicted worse iDFS highlights the real-world clinical reality that patients receiving NAC often present with more biologically aggressive disease. This suggests that recurrence risk may be underappreciated when decisions are based solely on treatment modality rather than underlying tumour biology and nodal burden. This finding is consistent with previous studies, which suggest that patients requiring NAC often present with more aggressive tumour biology or advanced disease stages, contributing to poorer outcomes. These results highlight the need for carefully considering additional adjuvant therapies, such as abemaciclib, in this subgroup to mitigate the elevated baseline risk.
The baseline characteristics of the patients in our cohort are closely aligned with those of the monarchE trial, including age, menopausal status, hormone receptor and HER2 status, and patterns of lymph node involvement. This alignment enhances the generalisability of our findings and supports the relevance of our analysis to clinical populations eligible for adjuvant abemaciclib therapy.
In the ITT population of MonarchE Cohort 1, the HR for iDFS was 0.680 (95% CI: 0.599–0.772), which indicates a considerable improvement in the abemaciclib group than endocrine therapy alone. The 5-year iDFS rates were 83.6% and 76.0% in the abemaciclib and endocrine therapy-alone groups, respectively, resulting in an absolute risk reduction of 7.6%. Although the N1 + >5 cm subgroup showed no significant difference from non-eligible patients in our cohort, this group still met the high-risk definition in the monarchE trial and demonstrated benefit from abemaciclib, underscoring the need to interpret eligibility in the context of individualized risk.
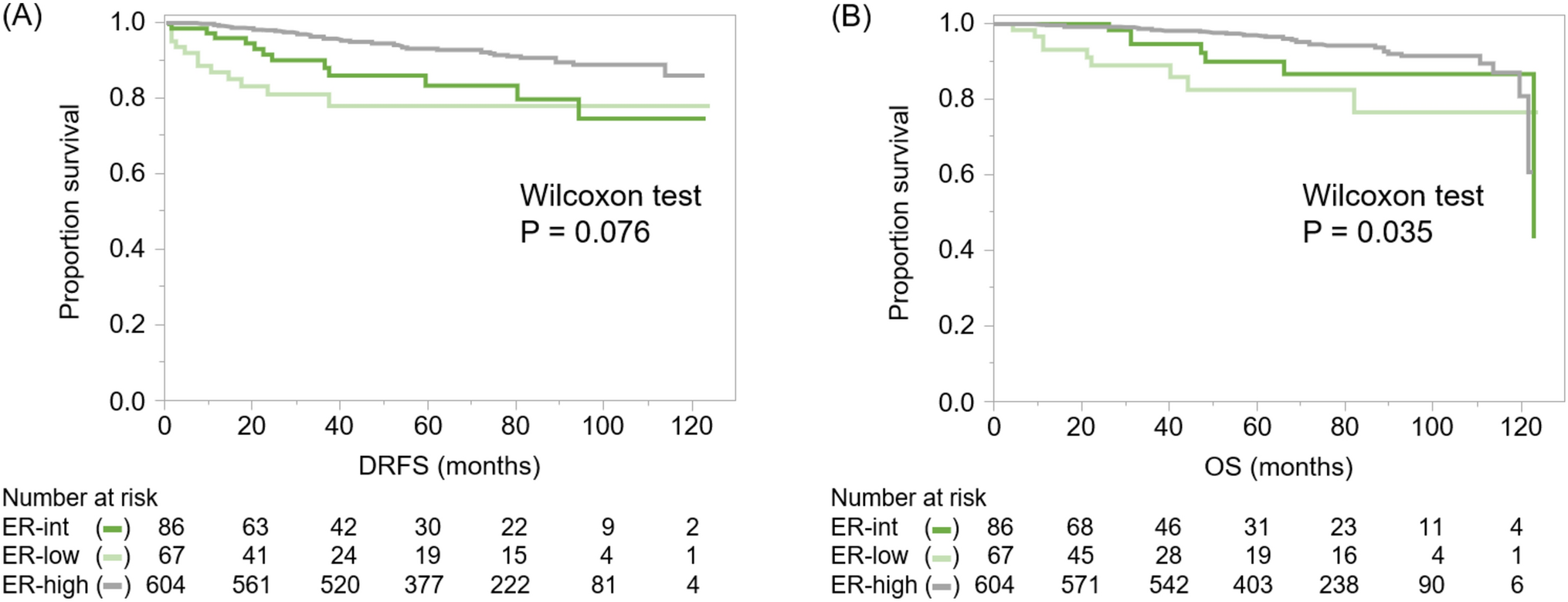
Overall, our findings suggest that the magnitude of absolute risk reduction achieved with perioperative abemaciclib therapy may vary depending on baseline recurrence risk among high-risk subgroups. Therefore, it is essential to calculate and discuss absolute risk reduction for each patient, considering their risk profiles. Shared decision-making with patients, based on a discussion of the risk–benefit balance, is crucial when considering the addition of abemaciclib therapy to endocrine treatment. In our cohort, the 5-year overall survival (OS) was 99.2% (95% CI: 98.6–99.8) in the non-eligible group, compared with 91.5% (86.2–97.2) in the eligible group. Similarly, the 5-year iDFS was 94.9% (93.4–96.5) and 80.1% (73.2–87.6), respectively. These values closely align with the control arm of the monarchE trial (5y OS: 89.6%, iDFS: 79.4%), underscoring the validity of the risk stratification even in a real-world setting.
Furthermore, recent surgical trials such as ACOSOG Z0011, AMAROS, and SENOMAC have shifted clinical practice toward de-escalation of axillary surgery in select patients [14,15,16]. However, our results—supported by monarchE and NATALEE—emphasize that treatment escalation in the adjuvant setting should still be considered based on individualized assessment of nodal burden and recurrence risk, even when surgical intervention is minimized.
These findings highlight the necessity of personalized risk stratification in determining the utility of adjuvant abemaciclib. Rather than applying trial eligibility criteria rigidly, clinicians should estimate absolute risk reduction on a patient-by-patient basis. Risk calculators or validated clinical prediction models, potentially combined with biomarkers such as ctDNA or MRD status, could facilitate more nuanced decisions [17]. Moreover, these individualized estimates of benefit should be transparently discussed with patients to support shared decision-making, particularly in light of the toxicities and financial costs associated with prolonged CDK4/6 inhibitor use.
This study has some limitations that should be considered when interpreting the findings. First, this was a retrospective analysis conducted at a single institution, which may limit the generalisability of the results to a broader population. Additionally, the study population consisted solely of Asian patients, which may limit the applicability of these findings to non-Asian populations, owing to potential ethnic and genetic differences in disease progression and treatment response. The reliance on medical records for patient data may also introduce potential biases owing to incomplete or inconsistent documentation. Furthermore, although our study closely mirrors the patient characteristics of the monarchE trial, differences in treatment approaches, follow-up protocols, and supportive care practices between institutions may have influenced the outcomes. Finally, some subgroups—such as those with N1 + >5 cm tumours—had relatively small sample sizes, limiting our ability to detect modest differences. Future multicentre prospective studies with larger, ethnically diverse populations are warranted to validate these findings and to better model baseline risk across the full spectrum of high-risk early breast cancer.
In conclusion, we assessed the baseline risk characteristics of patients with high-risk, HR-positive, HER2-negative early-stage BC using criteria aligned with the monarchE trial. Our findings demonstrated that distinct subgroups within this high-risk population have varying baseline prognoses, which may influence the absolute benefits of adjuvant abemaciclib therapy. These insights advocate for individualized risk assessment beyond categorical eligibility, and support a more tailored approach to the incorporation of CDK4/6 inhibitors in the adjuvant setting.

Comments (0)