To our knowledge, this paper is the first to provide evidence of differing carcinogenic processes in a patient with GDH for BRCA1 and BRCA2 between right and left breast cancer by somatic mutation analysis, expanding the target to the main tumor suppressor genes. Most importantly, breast carcinogenesis in HBOC with GDH for BRCA1 and BRCA2 depends on each mutation event in tumor suppressor genes, including BRCA1 or BRCA2, but not on common mechanisms in GDH carriers with both BRCA1 and BRCA2.
Seven cases with GDH for BRCA1 and BRCA2 were registered in JOHBOC (2020), corresponding to 0.5% of BRCA1 or BRCA2 pathogenic variant (PV) carriers (7/1364) [4]. The dataset of CIMBA, the International Research Consortium for HBOC, included 93 individuals (0.29%) from 84 families of 32,295 female carriers with BRCA1/2 PVs; of cases with GDH for BRCA1 and BRCA2, 45.2% were involved in three common germline PVs in Ashkenazi [11]. The frequency of BRCA1 and BRCA2 GDH carriers in our country is not as rare as that of foreign countries in CIMBA.
The germline BRCA1 variant, c.5193 + 2dup in the proband was classified as “likely pathogenic” in the BRACAnalysis® test report of the proband by Myriad. Recently, Ambry Genetics registered this variant in the ClinVar database as “pathogenic” based on their internal data that this variant results in abnormal splicing in the set of samples tested [12]. We confirmed their internal data by conducting RT-PCR analysis using total RNA prepared from cultured T cells of the proband treated with puromycin. When conducting an in silico prediction tool for splicing, the SpliceAI tool [13] gave a delta score of 0.96 in donor loss, strongly suggesting splicing alteration. SPiCE v2.1 [14] also predicted the loss of splicing donor, while Human Splicing Finder Pro (Genomnis, Marseille, France) demonstrated no significant impact on splicing signals. Thus, confirming the splicing alteration in the proband’s material was very important. We provide clear evidence that this variant induced the skipping of the entire exon 19 to generate aberrant RNA that was destroyed via a nonsense-mediated decay system in the peripheral blood cells. This finding supports the submission of Ambry Genetics at ClinVar based on their internal data.
Patients with GDH for BRCA1 and BRCA2 were first reported in a Hungarian HBOC family [15]. Clinical and pathological studies of breast cancers in Korean patients with GDH for BRCA1 and BRCA2 revealed that the age of onset was younger than that of patients with a single germline PV of BRCA1 or BRCA2 and the probands had a more dense family history of breast cancer [16]. Additionally, pathological findings in terms of estrogen and progesterone receptor status and dominance of triple-negative breast cancer among subtypes were similar to those with BRCA1 single PV [16].
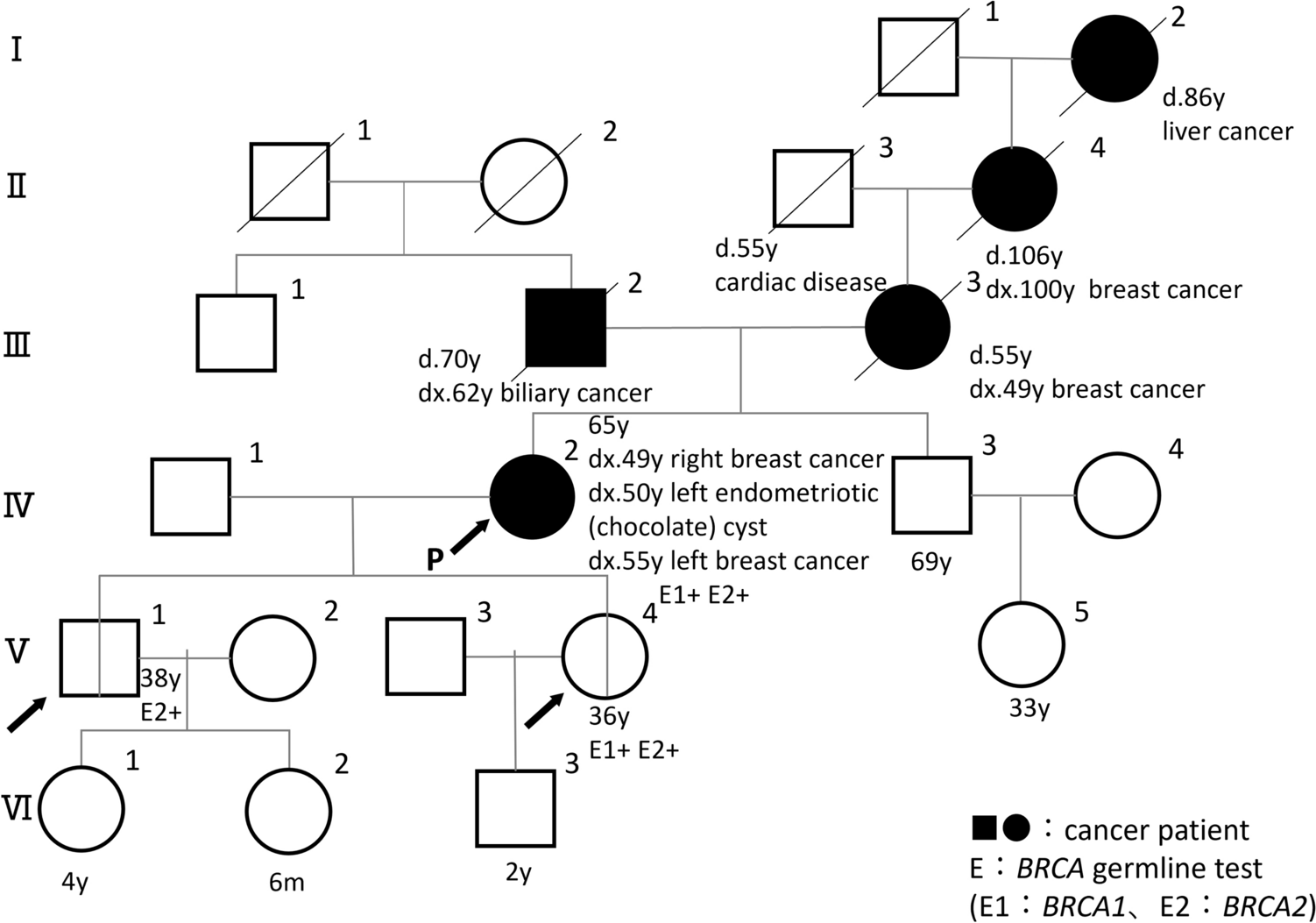
In the family of the proband, there are three patients with breast cancer: herself, her mother, and her maternal grandmother. Their onset age of breast cancer was 49, 49, and 100 years, respectively. The proband’s onset age was not less than the average age of a single germline pathological variant carrier (BRCA1: 40.2 years, BRCA2: 41.7 years) of Japanese patients with breast cancer with either BRCA1 or BRCA2 [1]. In contrast, the pathological findings of both bilateral breast cancers of the proband were triple negative, a typical characteristic of breast cancer with BRCA1 germline PV carriers. This was consistent with the findings of a previous study [16].
In this case, somatic mutation analysis in breast cancer tissue specimens demonstrated that the pathogenesis may differ between right and left breast cancer. Right breast cancer is associated with BRCA1 inactivation. In contrast, BRCA2 and APC, typical tumor suppressor genes, may be involved in left breast cancer carcinogenesis. A study examined the LOH of BRCA1 and BRCA2 in 12 breast and ovarian cancer specimens with GDH and concluded that there was no specific pattern in the two-hits status of BRCA1 and BRCA2 [11]. They reported that three cases (one BRCA1 and two BRCA2 cases) of breast cancer and one case in BRCA1 of ovarian cancer showed LOH, but they could not find any LOH in the remaining cases. In a Japanese breast cancer case with GDH for BRCA1 and BRCA2, immunohistochemical analysis of breast cancer tissue of the patient revealed loss of both BRCA1 and BRCA2 proteins; therefore, both alleles of BRCA1 and BRCA2 might simultaneously be inactivated [17]. In contrast, there were no cases of both inactivation of BRCA1 and BRCA2 in Rebbeck’s report [11]. In our case, each tumor had its own carcinogenesis process. Specifically, in the left breast cancer, APC inactivation was observed in addition to the BRCA2 inactivation. APC somatic mutation has been found in 18% of breast cancer cases; the mutations were significantly more frequent in higher, advanced stages, suggesting that APC mutations are associated with tumor progression in breast cancers [18]. Since some cases cannot be explained solely by two-hit events in the BRCA1 and BRCA2 genes [11], we extended the extent of target genes for two-hit to other main tumor suppressor genes. This enabled us to comprehensively show the left breast cancer carcinogenesis.
From our findings in this study, it revealed that two-hit event of tumor suppressor gene is not necessarily restricted to generate in an allele of causasive gene with a pathogenic variant. Germline genetic testing such as BRACAnalysis® may not reflect inactive status of the tumor suppressor gene in his or her tumor. Tumor acquired heterogeneity as it grows. It could be cause the discrepancy between the result of companion diagnosis and the effect of molecular targeted drugs.
As multi-gene panel testing becomes more widespread, the possibility that multiple pathogenic variants are detected will be enlarged in clinical practice. These variants are transmitted based on Mendelian inheritance. We should take care of the possibility that there remaind the existence of another pathological variant, if the clinical phenotype cannot be completely explained by the result of genetic testing, however, it is difficult in similar functional genes such as BRCA1 and BRCA2.
In conclusion, we present evidence of independent carcinogenesis of bilateral breast cancer developed in a Japanese patient with HBOC who harbored GDH for BRCA1 and BRCA2.

Comments (0)