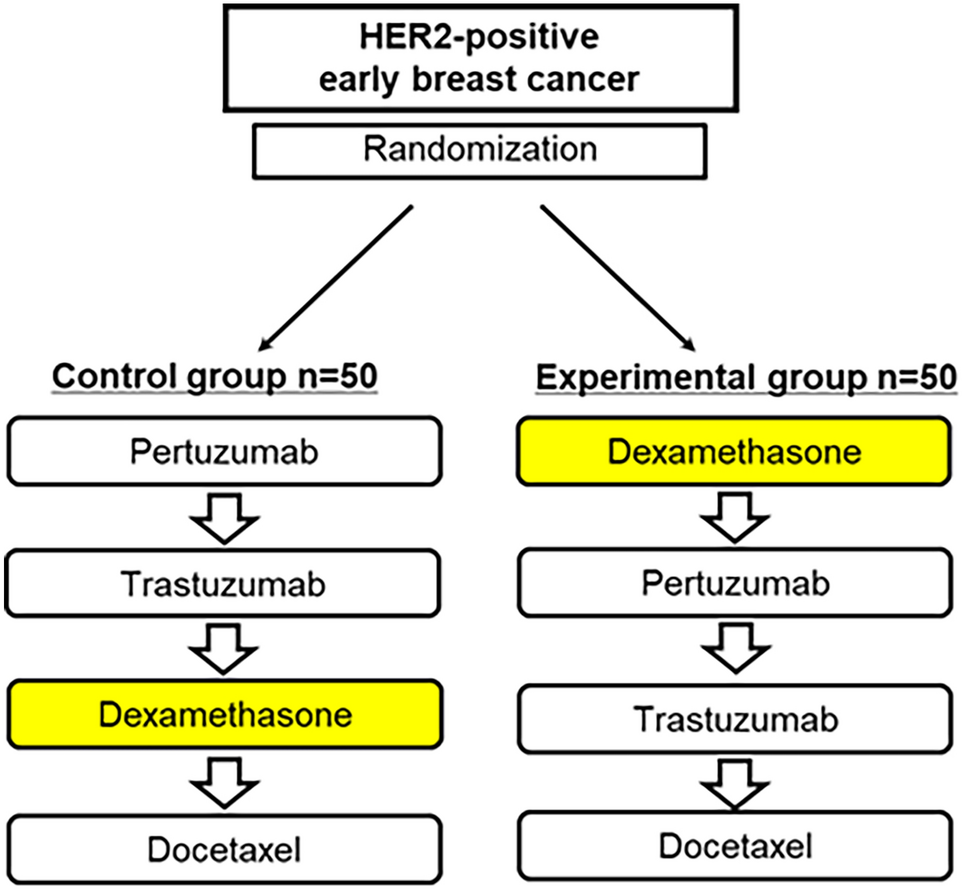
This randomized clinical trial demonstrates that modifying the sequence of dexamethasone administration significantly reduces the incidence of IRs in patients receiving HER2-targeted therapy for early-stage HER2-positive breast cancer. Specifically, administering dexamethasone before pertuzumab and trastuzumab significantly reduced the rate of IRs during cycle 1, compared to the standard sequence where dexamethasone is administered only before docetaxel. These findings support the hypothesis that earlier corticosteroid premedication confers protective benefits during biologic agent infusions, extending beyond its established role in cytotoxic chemotherapy.
There was a statistically significant and clinically meaningful 36% absolute reduction in IR incidence, from 60.0% to 24.0% (P < 0.05, 95% CI excludes zero). This result is consistent with previous retrospective studies indicating that early corticosteroid administration may reduce IRs associated with monoclonal antibody therapies [11,12,13,14,15]. However, this study represents the first prospective, randomized evidence supporting dual HER2 blockade using trastuzumab and pertuzumab. Notably, no grade ≥ 3 IRs were observed in either group. However, while most IRs were low-grade, they remained common and could disrupt treatment continuity and patient experience. This may reflect limited power to detect rare severe events. The modified premedication sequence may primarily reduce mild-to-moderate IRs, which still affect patient comfort and adherence. Larger studies are needed to assess its impact on severe IRs. Similarly, the lack of a significant difference in cycle 2 may be due to immune tolerance developed after initial exposure during cycle 1, leading to an overall lower baseline risk in subsequent cycles. Nevertheless, the possibility of insufficient power to detect small intergroup differences cannot be excluded. These findings underscore that the benefit of early dexamethasone administration is most pronounced during the first cycle.
Importantly, the benefit of the modified dexamethasone sequence was primarily observed during the first treatment cycle, when the immune system typically shows the strongest response to newly introduced monoclonal antibodies. In the second cycle, IR rates were low and comparable between treatment groups, consistent with the expected development of immune tolerance following initial exposure. This temporal pattern underscores the importance of optimizing premedication strategies, particularly during the initial administration of HER2-targeted agents.
Although the modified premedication sequence significantly reduced IRs—particularly chills, flushing, and vomiting—the overall incidence of TRAEs remained high and comparable between groups. This suggests that while the timing of dexamethasone administration effectively mitigates acute immune-related reactions commonly observed with monoclonal antibodies, it does not influence the broader toxicity profile of chemotherapy or HER2 blockade. These findings are reassuring from a safety perspective and offer practical insight into which IR components may be most responsive to premedication optimization.
A detailed time-course analysis showed that IRs in the control group occurred primarily during or immediately after pertuzumab and trastuzumab infusion—before dexamethasone administration. In contrast, IRs in the treatment group were less frequent and more evenly distributed across subsequent time points, suggesting that early corticosteroid administration effectively prevents acute IRs to HER2-targeted therapy. These findings have practical implications, suggesting that modifying the infusion order may serve as a simple yet effective strategy to improve patient comfort and treatment tolerability.
Although previous guidelines, including those from the European Society for Medical Oncology (ESMO), do not routinely recommend corticosteroid premedication for trastuzumab [13, 16], our findings suggest that a modified premedication regimen may provide significant clinical benefits.
These recommendations primarily address whether corticosteroids should be used for single-agent HER2-targeted therapy, but do not consider the timing of administration in combination regimens that include cytotoxic agents. Importantly, our study does not aim to reassess the necessity of steroids for trastuzumab monotherapy, but rather emphasizes the clinical relevance of modifying the sequence of administration when corticosteroids are already indicated—for example, for docetaxel—to enhance protection against early-onset IRs. Furthermore, our findings are consistent with prior studies of monoclonal antibodies such as cetuximab and rituximab, for which corticosteroid premedication has been shown to reduce hypersensitivity reactions [3, 17]. This trial extends those insights to HER2-targeted regimens, highlighting the critical importance of steroid timing in mitigating IRs.
Furthermore, the implications of this study may extend beyond HER2-positive breast cancer. IRs are a common adverse effect of monoclonal antibody-based therapies, which are widely used in both oncologic and non-oncologic diseases [3]. Agents, such as immune checkpoint inhibitors (e.g., pembrolizumab, nivolumab) and anti-cluster of differentiation 20 (anti-CD20) monoclonal antibodies (e.g., rituximab) are associated with high rates of IRs [18, 19]. For these therapies, optimizing premedication strategies—particularly the timing of corticosteroid administration—may improve tolerability, minimize treatment interruptions, and improve patient adherence.
In this study, no patients received oral dexamethasone prior to treatment. All patients were administered intravenous dexamethasone (6.6 mg) on the day of infusion as per protocol, and oral dexamethasone was prescribed for two days after treatment to prevent docetaxel-induced edema. Antipyretic or analgesic agents such as acetaminophen and NSAIDs were also not included in the premedication protocol. In Japan, prophylactic use of these agents for infusion reaction prevention in this context is considered off-label, and their use may vary across institutions. While these agents may be used at the discretion of clinicians, their potential role—either in combination with or as an alternative to corticosteroid premedication—was beyond the scope of this trial.
Therefore, the observed reduction in infusion reactions in our study can be attributed to the timing of intravenous dexamethasone administration on the day of treatment. Future studies may further investigate these adjunctive strategies, although their necessity should be weighed against current clinical practices and the established efficacy of steroid-based approaches.
No association was found between baseline laboratory parameters (white blood cell counts, NLR, liver enzymes, and renal function) and the development of IRs. This finding suggests that routine blood tests may have limited clinical utility in predicting IR risk. Instead, focusing on modifiable factors—particularly premedication protocols—may provide a more effective preventive strategy.
This study has several limitations. First, while the sample size was sufficient to detect differences in IR rates, it may not have been adequately powered to detect differences in less frequent adverse events or within specific patient subgroups. Second, the study population comprised exclusively patients with early-stage disease receiving standard perioperative therapy; consequently, the findings may not be generalizable to metastatic settings or patients receiving alternative HER2-targeted treatments. However, this curative-intent setting represents a critical context in which treatment tolerability is essential. This trial therefore provides definitive guidance for optimizing premedication protocols in early-stage HER2-positive breast cancer, while highlighting the need for further research in metastatic disease. Third, the assessment of IRs relied solely on clinical symptoms and timing, without incorporating biomarkers or mechanistic assays to characterize the underlying immune response. In addition, a numerically higher incidence of grade ≥ 3 adverse events was observed in the experimental group. However, this analysis was based on the secondary endpoints that were not powered for formal statistical comparison, and multiple safety outcomes were explored without adjustment for multiplicity. Therefore, this finding should be interpreted with caution, as it may reflect random variation rather than a true difference in toxicity between groups. Finally, while there were no missing data for predefined endpoints, some minor or subjective symptoms may not have been consistently reported across sites. Despite the use of standardized CRFs, a minimal risk of underreporting remains, which is an inherent limitation in multicenter data collection.
Regardless of these limitations, the study demonstrates that optimizing dexamethasone timing represents a practical, cost-effective strategy for reducing IRs in patients receiving trastuzumab and pertuzumab therapy. Based on these findings, modifying institutional premedication protocols to include dexamethasone prior to HER2-targeted therapy—particularly during the first treatment cycle—may be feasible. This approach’s simplicity and potential applicability to other monoclonal antibody therapies highlights its relevance across diverse clinical settings.

Comments (0)