In this real-world study of women with HR +/HER2 − ABC in Japan, neither palbociclib plus ET nor ET alone had any substantial detrimental impacts on HRQOL, based on patient assessment using the ePRO system, and PA, as measured by a wearable device. This is the first real-world study to assess the impact of palbociclib plus ET or ET alone on both HRQOL and PA metrics in women with HR +/HER2 − ABC in Japan. Although our study duration was limited to 24 weeks, the fact that palbociclib plus ET or ET alone did not lead to detriments in HRQOL is notable considering HRQOL scores, measured with the EORTC QLQ-C30 or similar tools, and PA typically decline with disease progression and/or treatment in patients with BC [30, 31]. Our study findings are consistent with those of the PALOMA clinical trials [17, 18], and add to the existing evidence that CDK4/6 inhibitors, including palbociclib, in combination with ET maintain HRQOL among patients with ABC as reported in a systematic review of 31 clinical trials and 7 real-world studies [22].
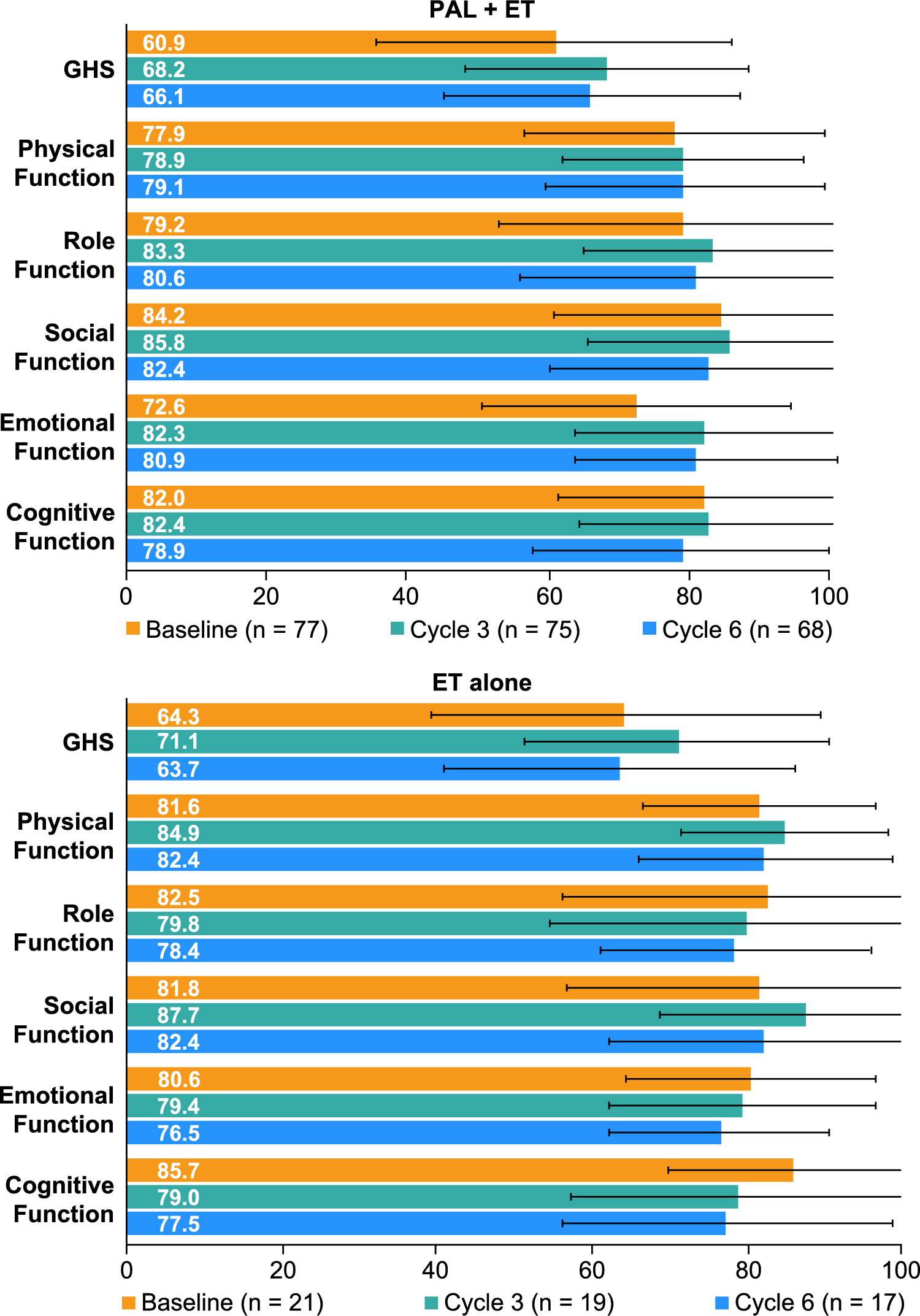
Among the patients who received palbociclib plus ET, GHS scores averaged 60.9 prior to treatment initiation and 66.1 in the 6th cycle of treatment. Among those patients who received ET alone, GHS scores averaged 64.3 and 63.7, respectively. These GHS scores are similar to those reported in PALOMA-3, in which post-treatment GHS score was to some extent higher in patients who received palbociclib plus fulvestrant versus those who received placebo plus fulvestrant (66.1 vs 63.0; P = 0.0313) [18]. Clinical trial HRQOL data are typically captured at Day 1 of a treatment cycle and post-treatment [18]. In this study, PROs were assessed on Day 15 of 6 treatment cycles, thereby providing real-world evidence of patients’ perspectives of their HRQOL while on treatment with palbociclib plus ET.
Guidelines/policies of the European School of Oncology and European Society for Medical Oncology, the ABC Global Alliance, United States Centers for Medicare & Medicaid Services Enhancing Oncology Model, and the PRO working group of the Japanese Association of Supportive Care in Cancer have prioritized the incorporation of validated PRO assessments into oncology research and routine patient care [14, 16, 32, 33]. In addition, it is internationally recognized that electronic monitoring of PROs and real-time data collection has great utility for facilitating communication with patients and care teams, decision-making, and early intervention, all of which are aimed at improving patient overall QOL [14, 16, 32]. Basch and colleagues conducted a seminal randomized controlled trial in the United States that showed that electronic symptom reporting among 766 patients with advanced cancers (breast, genitourinary, gynecologic, and lung) improved HRQOL, reduced emergency and hospital visits, increased time on chemotherapy, and prolonged survival [34, 35]. PRO measures of HRQOL represent key secondary outcomes of oncology research and are particularly important among patients with ABC considering they are living longer in many countries throughout the world, including Japan, but still have an incurable disease [13, 36, 37]. Systematic assessments of how patients function and perform daily activities while on palbociclib plus ET is informative of treatment effectiveness, safety, and tolerability from the patient perspective. Such observational, less burdensome patient data collection may be of high value for clinical decision-making and the timely individualization of patient care for ABC.
Another emerging and increasingly important measurement in oncology research is PA, and wearable devices are progressively being chosen for more objective measurement of patients’ PA activity relative to self-reported estimates [19, 38]. In the current study, at baseline, sedentary time averaged 581 min/day (9.7 h/day) among patients who initiated palbociclib plus ET and 513 min/day (8.6 h/day) among those who initiated ET alone. Over the course of 6 cycles of treatment, sedentary time did not considerably change in either treatment group, which was similarly observed for other PA metrics, including moderate-to-vigorous PA, steps, and light PA. In a literature review of oncology clinical trials in which wearable activity monitors were utilized by patients with cancer (n = 41 trials; 65% BC; 63% post-treatment; 37% patients with active cancer, sedentary time ranged 413 to 556 min/day (n = 6 trials) [19]. Thus, the patients included in the current study had generally similar sedentary behavior as other patients with cancer [19]. For comparison of sedentary time with a general population in Japan, among a large study of 36,023 women aged 35 to 69 years (Japan Multi-Institutional Collaborative Cohort Study, 2004–2014), 47.5% spent < 10 h/day sedentary, while 52.5% spent 10 to ≥ 13 h/day sedentary based on patient survey responses [39]. Maintaining or increasing PA may be especially important for patients with BC in Japan, considering women in Japan spend more time sedentary compared with other populations, which increases their susceptibility to BC [39]. The World Health Organization guidelines on PA and sedentary behavior strongly recommend adults (18─64 years of age) should limit the amount of time spent being sedentary and replace this time with PA of any intensity to yield health benefits [40].
In a meta-analysis that evaluated the association of PA with mortality and the influence of intensity, moderate and high intensity PA post-diagnosis versus low amount of PA, were associated with 31% and 42% significant reductions, respectively, in BC-specific mortality, while decreased PA post-diagnosis was associated with the greatest mortality risk [21]. In a feasibility, single-arm clinical trial of patients with ABC treated with chemotherapy, hormone therapy, or targeted therapy (Advanced stage Breast cancer and Lifestyle Exercise [ABLE]; n = 49) conducted in France, a personalized PA program that included monitoring with a wearable device was found to improve physical outcomes (eg, decreased sitting time, increased 6 min walking distance), while fatigue decreased by 16%, although this was not statistically significant; GHS and functional domain scores of the EORTC QLQ-C30 QOL remained stable [41]. Although not in the scope of the current study, it will be important future research evaluates whether interventions to increase PA among patients with ABC treated with palbociclib plus ET improves HRQOL and prolongs survival.
The findings of this study should be interpreted in the context of its strengths and limitations. The real-world observational design of this study had potential for missing data, which may have been more apparent with the measurement of ePROs. However, ePRO assessments were done repeatedly on Day 15 throughout 6 cycles of treatment, with 95% of patients completing the 6-cycle observation period. Therefore, the data may be more comprehensive than in studies in which such measurements are only completed at the beginning and end of treatment. Also, compliance with ePRO assessment completion was relatively high in the study groups. In this study, PA was measured objectively and longitudinally in real-time with a wearable device and the PA metric data may be more dependable than self-reported survey estimates, which may under- or over-estimate PA metrics; additionally recall bias was avoided [19, 39]. Moreover, PA metric data were collected weekly for 24 weeks, thereby providing relatively continuous estimates of multiple PA types over the course of treatment for ABC.
For this study, ePRO data were captured via a smartphone-based ePRO system, and participating patients must have had some experience with this technology. Those patients with less technological mobile device skills were likely underrepresented. Furthermore, the patients enrolled were willing to complete data collection and wear the wearable device. They also had an ECOG PS of 0 or 1. Thus, the patients may represent a more knowledgeable, engaged and healthier set of patients. This study had a small sample size, the observation period was 24 weeks, and only women from Japan were included. Patient selection, treatments received, and monitoring procedures were based on the discretion of the treating physician in routine clinical practice; thus, there is a potential for selection and responder bias. Between- and within-group comparisons were not performed due to the study design, which was not aimed to show superiority or inferiority, and did not have a sample size calculation. Only associations, not causality, can be inferred between treatments and outcomes due to the observational nature of this study. Lastly, the observational period may have resulted in a seasonal effect on PA. Despite the seasonal variations, the pace of patient enrollment remained relatively constant.

Comments (0)