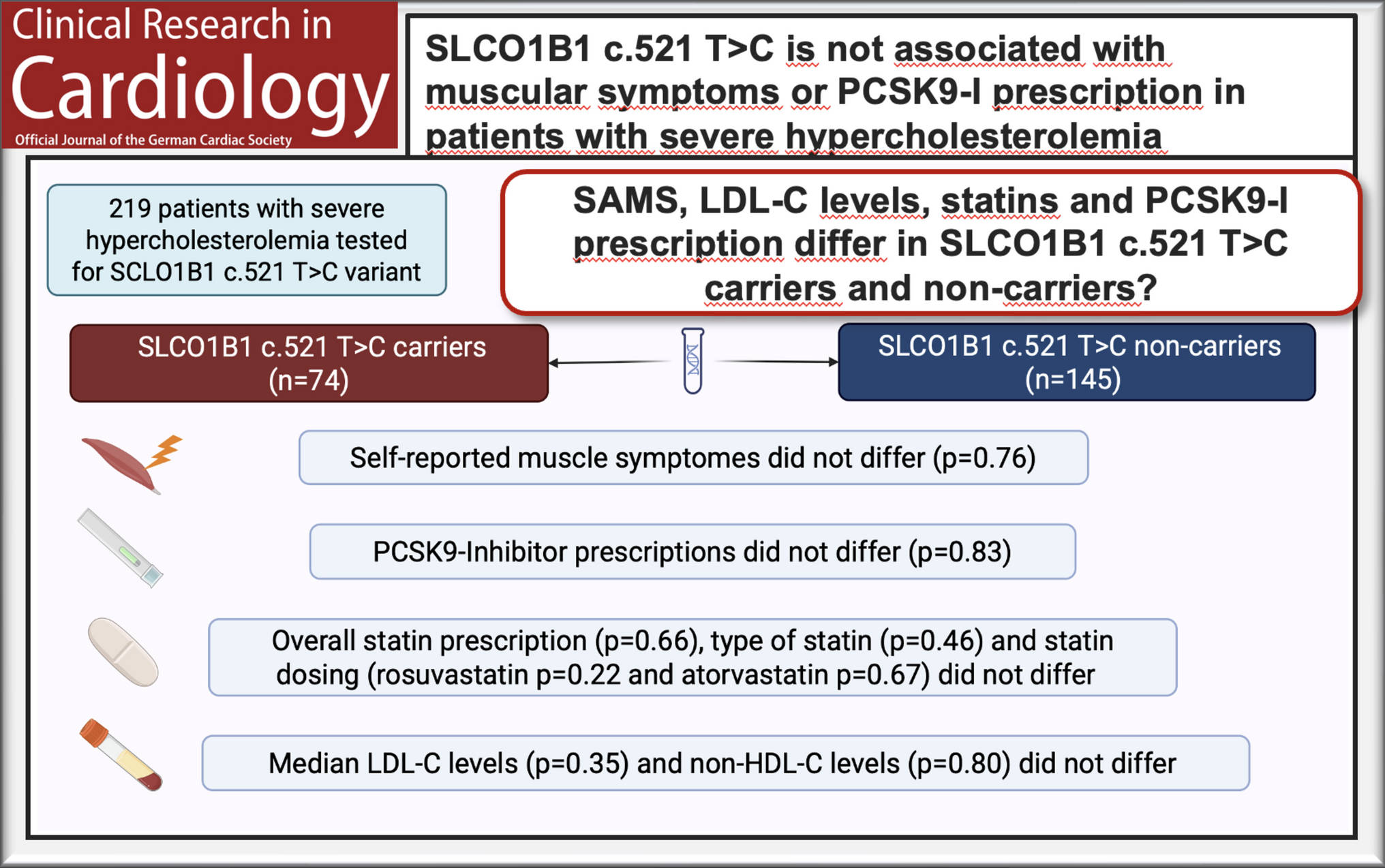
In this study, we investigated a cohort of patients with severe hypercholesterolemia to determine the association between SAMS and the rs4149056 variant of the SLCO1B1 gene (SLCO1B1 c.521 T > C). We were able to investigate 219 patients who were tested for FH and SLCO1B1 c.521 T > C. Although rates of self-reported SAMS and SLCO1B1 c.521 T > C were high, with 26.9% and 33.8%, respectively, we did not find any association between SLCO1B1 c.521 T > C variant and the occurrence of SAMS. The relatively high prevalence of SAMS in our cohort likely reflects referral bias inherent to a tertiary lipid clinic specializing in high-risk patients who fail to achieve LDL-C targets, rather than the prevalence of statin intolerance in the general population. Notably, patients were treated exclusively with rosuvastatin or atorvastatin, indicating that the SLCO1B1 c.521 T > C variant may have limited clinical relevance for SAMS under contemporary statin therapy. Furthermore, patients carrying this variant did not receive fewer statins or lower statin doses. Crucially, this is the first study to investigate PCSK9 inhibitor prescription as an alternative to statins in relation to SAMS and the SLCO1B1 c.521 T > C variant, showing no increased use in carriers.
The SLCO1B1 c.521 T > C variant (rs4149056) was initially identified as having a pharmacokinetic influence on simvastatin in 2006, and a strong association was subsequently found with myopathy in simvastatin-treated patients in 2008 [9, 11]. Since then, a similar relationship with atorvastatin has shown mixed results [17, 21], and rosuvastatin has shown no association in patients of European descent [15].
In an effort to deliver robust evidence for the association of SLCO1B1 c.521 T > C with SAMS, the ODYSSEY Outcomes Trial was one of the largest randomized controlled trials investigating this subject, in which an association between the SLCO1B1 c.521 T > C variant and SAMS could not be observed in patients treated with atorvastatin or rosuvastatin, respectively [16]. Furthermore, a recent meta-analysis found only a marginal excess rate of mostly mild muscle symptoms in large randomized controlled statin trials, questioning the significance of muscle symptoms in general [7]. However, despite the publication of those robust results in 2022, several studies have been published that further investigate the pharmacogenetic influence of the SLCO1B1 c.521 T > C variant and its relationship to SAMS [19, 22, 23]. As A. Gougeon et al. demonstrated, there may be evidence that some of these findings are subject to publication bias, thereby questioning the validity of those results [18]. This recent study assessed potential publication bias by applying the Robust Bayesian Meta-Analysis model to six systematic reviews including a total of 19 studies (8 cohort, 11 case–control). After assessing publication bias and correcting the odds ratio, they found no association between the SLCO1B1 c.521C > T variant and SAMS, and also no association when analysing statin subgroups or single nucleotide polymorphism type subgroups. Possibly the most important message behind this publication is the hypothesis that studies showing negative results may be underrepresented in the published literature, leading to an overestimation of positive findings. It is interesting that even simvastatin, on which the association of SLCO1B1 c.521C > T and SAMS was first discovered, showed negative results after correcting for publication bias. As this warrant more conclusive evidence from real-life clinical settings, our findings support previous data showing no correlation between SAMS and the SLCO1B1 c.521 T > C variant under atorvastatin or rosuvastatin treatment. It is important to note that our results only apply to patients treated with either atorvastatin or rosuvastatin and no other statin. Therefore, it has to be noted that these findings cannot be extrapolated to simvastatin-treated populations, where the strongest genetic associations were originally observed.
As described in the Results section, treatment with a PCSK9 inhibitor was more common among patients with self-reported SAMS (57.7%) than among those without SAMS (21.9%). In patients reporting SAMS, statin intolerance or reluctance to continue statin therapy may have limited the ability to achieve guideline-recommended lipid targets with oral therapy alone. Consistently, both statin prescription rates and statin dosages were lower in the SAMS group, thereby increasing the need of PCSK9 inhibitor use.
This gene variant is common, with an estimated c.521C allele frequency of approximately 18% in the general European population and 17.7% in the general Austrian population [24, 25]. In our cohort, the variant was observed more frequently (33.8%). A plausible explanation is referral bias inherent to the tertiary care setting. Our outpatient clinic specializes in patients at high cardiovascular risk who fail to achieve LDL-C targets, and as mentioned above 27% of the cohort reported SAMS, with an even larger proportion referred due to suspected statin intolerance. It is therefore likely that some patients—particularly those who developed SAMS while receiving simvastatin, which has been shown to be associated with an increased risk of SAMS in carriers of this polymorphism—were preferentially referred to our tertiary center. Notably, when contemporary statins were used, no relevant differences were observed, suggesting that the enrichment of the variant in our cohort may reflect historical prescribing patterns rather than a persistent pharmacogenetic effect under current treatment strategies.
Interestingly, in our study population, the prevalence of diabetes was slightly higher among carriers of the SLCO1B1 c.521 T > C variant (12.9% vs. 4.3%). However, a history of diabetes appeared to have little, if any, influence on the therapy regimen, as all individuals were evaluated for suspected familial hypercholesterolemia and were therefore managed as high cardiovascular risk patients. Due to the low absolute number of participants with diabetes, sensitivity or stratified analyses would have been underpowered and were therefore not performed. Consensus papers like the European Atherosclerosis Society Consensus Panel Statement on SAMS name diabetes as a potential risk factor for developing SAMS. Notably, previous evidence from randomized controlled trials suggests no meaningful difference in the occurrence of statin-associated muscle symptoms between patients with and without diabetes, at least in low to moderate intensity statin regimes [7].
Given the reduced hepatic statin uptake associated with the SLCO1B1 c.521 T > C variant, one might expect that mutation carriers would exhibit reduced statin efficacy and therefore higher levels of LDL-C. However, in our population, there was no significant difference in LDL-C levels between genotype groups. This finding can be explained by several factors. First, the impact of SLCO1B1 c.521 T > C on statin efficacy is statin-specific, with the most pronounced effect observed for simvastatin. Meta-analyses demonstrate that the c.521C allele significantly reduces LDL-C lowering efficacy for simvastatin and pravastatin in non-Asian populations, while the effect on atorvastatin efficacy is less consistent [26, 27]. For rosuvastatin, although the SLCO1B1 polymorphism affects pharmacokinetics and can reduce lipid-lowering response, the magnitude of this effect appears more modest compared to simvastatin [28]. In our cohort, all patients were treated with atorvastatin or rosuvastatin but not simvastatin, which would substantially attenuate any genotype-related differences in LDL-C outcomes.
Second, most patients in our population were treated with combination lipid-lowering therapy rather than statin monotherapy. When ezetimibe or PCSK9 inhibitors are added to statin therapy, they provide substantial additional LDL-C reduction independent of statin pharmacogenetics. These non-statin agents act through mechanisms independent of OATP1B1-mediated hepatic uptake, thereby compensating for any possible reduced statin efficacy in SLCO1B1 variant carriers. Consequently, even if variant carriers experience modestly reduced statin efficacy, the addition of ezetimibe or PCSK9 inhibitors would minimize or eliminate genotype-related differences in final LDL-C concentrations.
One aspect of our findings that requires attention is the lower prescription rate of ezetimibe in SAMS patients within our study population. We hypothesize that in a clinical setting, patients who experience muscle symptoms may exhibit similar symptoms to those caused by ezetimibe due to a nocebo effect. In addition, ezetimibe may be discontinued along with statins in patients with muscular symptoms, as both medications are commonly prescribed together in a single pill.

Comments (0)