
Remember me
A total of 3360 patients that underwent TAVI at the Department of Cardiology at TUM University Hospital German Heart Centre (derivation cohort) between January 2014 and December 2023 were screened for inclusion. After exclusion, a total of 1254 patients with complete and available SII values were included in the analysis of the derivation cohort (n = 418 in the low tertile, n = 418 in the intermediate tertile and n = 418 in the high tertile) (Fig. 1).
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Inclusion and exclusion criteria (derivation cohort). SII = Systemic Immune-Inflammation Index
Derivation cohortBaseline, laboratory, and echocardiographic characteristics of the study population are summarized in Table 1. Median SII value for the overall cohort was 908 [581; 1486], for the low tertile 475 [363; 581], for intermediate tertile 908 [789; 1047], and for high tertile 1853 [1486; 2739]. The mean age was 81.8 [77.7; 85.1] years (low tertile: 81.6 [77.7; 85.1] years, intermediate tertile: 81.3 [77.3; 84.4] years, high tertile: 82.6% [79.5; 85.9] years, p < 0.001) and 43.9% were female [low tertile: 38.3%, intermediate tertile: 40.9%, high tertile: 52.4%, p < 0.001]. NYHA class III/IV (overall: 52%, low tertile: 46.2%, intermediate tertile: 49.2%, high tertile: 61.2%, p < 0.001) and CRP levels (overall 2.87 [1.41; 7.69] mg/L, low tertile 2.13 [1.16; 5.36] mg/L, intermediate tertile 2.82 [1.45; 6.58] mg/L, and high tertile 4.06 [1.66; 14.0] mg/L, p < 0.001) were higher in the higher tertile.
Table 1 Baseline characteristics of the derivation cohortProcedural characteristics are shown in Table 2. Device success was similar among tertiles (overall: 89.6%, low tertile: 89.7%, intermediate tertile: 89.5%, high tertile: 89.7%, p = 0.991), with higher incidence of tamponade in the higher tertile (overall 1.04%, low tertile 0.24%, intermediate tertile 0.72%, high tertile 2.15%, p = 0.017), but no difference regarding annulus rupture, coronary impairment or vascular complication. ICU stay were slightly higher in higher tertile (overall 1.00 [1.00; 1.00], low tertile 1.00 [1.00; 1.00], intermediate tertile 1.00 [1.00; 1.00], and high tertile 1.00 [1.00; 2.00], p = 0.015).
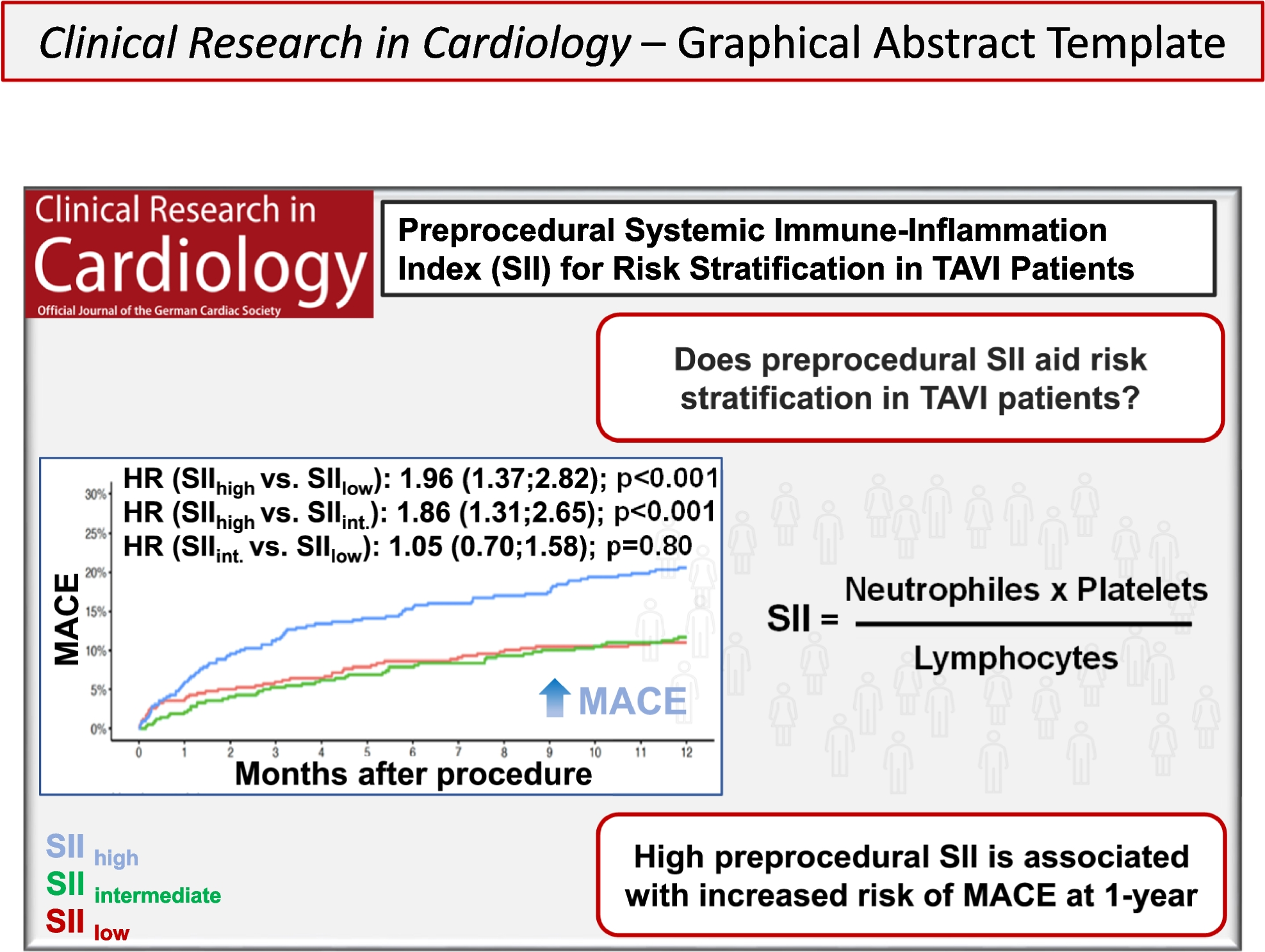
Table 2 Procedural characteristics of the derivation cohortSII and primary endpoint (MACE)MACE at one-year are shown in Table 3. MACE was higher in higher tertile when compared to low or intermediate tertiles (overall: 14.4%, low tertile: 11.0%, intermediate tertile: 11.7%, high tertile: 20.6%, p < 0.001). Kaplan–Meier curves showed that high tertile was associated with 86% increased risk of MACE when compared to intermediate [hazard ratio (HR) 1.86, 95% confidence interval (CI) [1.31, 2.65]; p < 0.001)] and 96% increased risk of MACE when compared to low tertile (HR 1.96, [1.37; 2.81, p < 0.001]) at one-year (Fig. 2A).
Table 3 Association between tertile-based Systemic Immune-Inflammation Index (SII) and clinical outcomes following transcatheter aortic valve implantation (TAVI) in the derivation cohortFig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Kaplan–Meier curves of one-year outcomes (A: MACE, B: all-cause death, C: stroke, D: CHF) according to the systemic immune-inflammation index (SII) (tertile-based analysis) prior to transcatheter aortic valve implantation (TAVI) in the derivation cohort. CHF = hospitalization for heart failure. MACE = Major Adverse Cardiac Event. HR = hazard ratio
In the multivariable cox regression analysis, adjusted for neutrophils, age, left ventricular ejection fraction (LVEF), aortic mean gradient, hemoglobin, creatinine, CRP, diabetes, peripheral artery disease (PAD), atrial fibrillation and type of valve, the association between SII and MACE in the tertile-based model narrowly missed statistical significance (SII high tertile vs SII intermediate tertile: HR 1.47, [0.99; 2.18], p = 0.056), (Table 3). However, when analyzed as a continuous variable, SII remained a significant predictor (HR 1.0001, [1.00001; 1.00002], p = 0.020), (Table 4). In the multivariable analysis of the individual components of the SII, the high neutrophiles tertile was associated with 58% increased risk of MACE compared to the intermediate tertile (HR 1.58 [1.07; 2.32], p = 0.022) (SupplementalTable 1). High platelets tertile and high lymphocyte tertile were not associated with increased risk of MACE compared to the intermediate tertiles (HR 1.17 [0.50; 1.15], p = 0.441 and HR 1.02 [0.67; 1.57], p = 0.915, respectively) (Supplemental Table 2 and Supplemental Table 3).
Table 4 Association between continuous value of Systemic Immune-Inflammation Index (SII) and clinical outcomes after TAVI at one-year in the derivation cohortAdditionally, individual variables as age ≥ 75 years (HR 1.91, [1.43; 2.56], p = 0.7061), female gender (HR 2.02, [1.29; 3.17], p = 0.8115), diabetes (HR 1.94, [1.19; 3.16], p = 0.9072), CAD (HR 1.71, [1.23; 2.39], p = 0.2578), NYHA III/IV (HR 1.90, [1.32; 2.73], p = 0.5666)), atrial fibrillation (HR 2.08, [1.42; 3.05], p = 0.4007) and EuroScore > 3.57 (HR 2.00, [1.40; 2.84], p = 0.3054) were associated with increased risk of MACE at one-year (Supplemental Fig. 1).
SII and secondary endpoints (all-cause mortality, stroke and CHF)Secondary endpoints are shown in Table 3. All-cause mortality was higher in higher tertile (overall: 10.3%, low tertile: 7.66%, intermediate tertile: 8.37%, and high tertile: 14.8%, p = 0.001). Kaplan–Meier curves showed that high tertile was associated with 85% increased risk of all-cause mortality compared to intermediate (HR 1.85 [1.22; 2.80], p = 0.004) and double the risk compared to low tertile (HR 2.00 [1.31; 3.07], p = 0.001) (Fig. 2B).
In multivariable cox regression analysis the association between SII and all-cause mortality was not statistically significant after adjustment for the above mentioned variables [tertile-based model (SII high vs SII low, HR: 1.30, [0.80; 2.10]; p = 0.284; SII high vs SII intermediate, HR: 1.28, [0.81; 2.02], p = 0.289) (Table 3), as continuous variable (HR 1.0001, [0.9999; 1.0001], p = 0.273) (Table 4). In the multivariable analysis of the individual components of the SII, the high neutrophiles tertile, the high platelets tertile and the high lymphocyte tertile were not associated with increased risk of all-cause mortality compared to the intermediate tertiles (HR 1.52 [0.97; 2.40], p = 0.069, HR 1.11 [0.69; 1.78], p = 0.0667 and HR 1.16 [0.69; 1.95], p = 0.570 respectively) (Supplemental Table 1, Supplemental Table 2 and Supplemental Table 3).
Age ≥ 75 years was associated with 92% increased risk of all-cause mortality (HR 1.92 [1.36; 2.72], p = 0.7583), male gender with 1.2 times increased risk (HR 2.18, [1.39; 3.40], p = 0.5412), diabetes with 92% increased risk (HR 1.92 [1.09; 3.38], p = 0.95), CAD with 86% risk (HR 1.86 [1.26; 2.73], p = 0.8260), NYHA III/IV with 99% risk (HR 1.99 [1.28; 3.10], p = 0.5387), atrial fibrillation with 1.2 times risk (HR 2.26 [1.44; 3.54], p = 0.2091) and EuroScore > 3.57 with 92% risk (HR 1.92, [1.28; 2.89], p = 0.5148) (Supplemental Fig. 2).
Stroke was higher in higher tertile when compared to low and intermediate (overall: 2.31%, low tertile: 1.20%, intermediate tertile: 1.67%, high tertile: 4.07%, p = 0.013). Kaplan–Meier curves showed that high tertile was associated with 1.5 times increased risk of stroke compared to intermediate (HR 2.52 [1.04; 6.07], p = 0.039) and 2.5 times increased risk compared to low tertile (HR 3.48 [1.29; 9.44], p = 0.014) (Fig. 2C). In multivariable cox regression analysis, the high SII tertile was associated with 2.6 times increased risk of stroke compared to intermediate (HR 3.67 [1.11; 12.16], p = 0.033) and 1.7 times increased risk compared to low tertile (HR 2.73 [0.97; 7.75], p = 0.058) (Table 3). When analyzed as continuous variable, the association of SII with increased risk of stroke remained significantly (HR 1.003 [1.0002; 1.0004], p < 0.001) (Table 4).
CHF hospitalization was higher in the higher tertile (overall: 4.70%, low tertile: 3.59%, intermediate tertile: 3.59%, high tertile: 6.94%, p = 0.031). Kaplan–Meier curves showed that high tertile was associated with 1.0 increased risk of stroke compared to intermediate (HR 2.02 [1.09; 3.77], p = 0.026) and 99% increased risk to low tertile (HR 1.99 [1.07; 3.72], p = 0.030) (Fig. 2D). In multivariable cox regression analysis, the high tertile was not associated with increased risk of CHF compared to intermediate (HR 1.56 [0.75; 3.24], p = 0.230) and low terile (HR 1.11 [0.53; 2.34], p = 0.774) (Table 3). When analyzed as continuous variable, no association was observed (HR 0.9999 [0.9998; 1.0001], p = 0.400) (Table 4).
Predictors of SIIAfter GLM analysis, only age (estimates 16.14, p = 0.013) and CRP (estimates 23.31, p < 0.001) were positively associated with SII whereas lower AS mean gradient (estimates −7.24, p = 0.022), while Hb (estimates −60.86, p = 0.011) was negatively associated with SII (SupplementalTable 4).
Validation cohort and one-year outcomesThe validation cohort comprised 568 patients from the Department of Cardiac Surgery, German Heart Center Munich, who underwent TAVI between January 2014 and December 2023, for whom a complete SII was available. The median age was 81.0 [76.8; 84.8] years, and 47.0% were female.
After ROC analysis, a value of 1204 was identified as the best discriminatory cut-off value for SII and patients were divided into two groups: Patients with a value of < 1204 (n = 293) were assigned to low risk and patients with a value > 1204 (n = 275) were assigned to high risk. Patients with a high SII were slightly older than those with a low SII (81.3 [77.0; 85.5] years versus 80.4 [76.5; 83.9] years, respectively, p = 0.045). Sex distribution was similar between groups: 45.1% females with low SII and 49.1% with high SII (p = 0.379). Adjusted Cox-proportional hazard model showed an increased risk for one-year all-cause mortality with high SII (HR 2.19 [1.59; 3.02], p < 0.001, Supplemental Fig. 3) and an increased risk for CHF (HR 1.76 [1.27; 2.44], p < 0.001, Supplemental Table 5).
Comments (0)