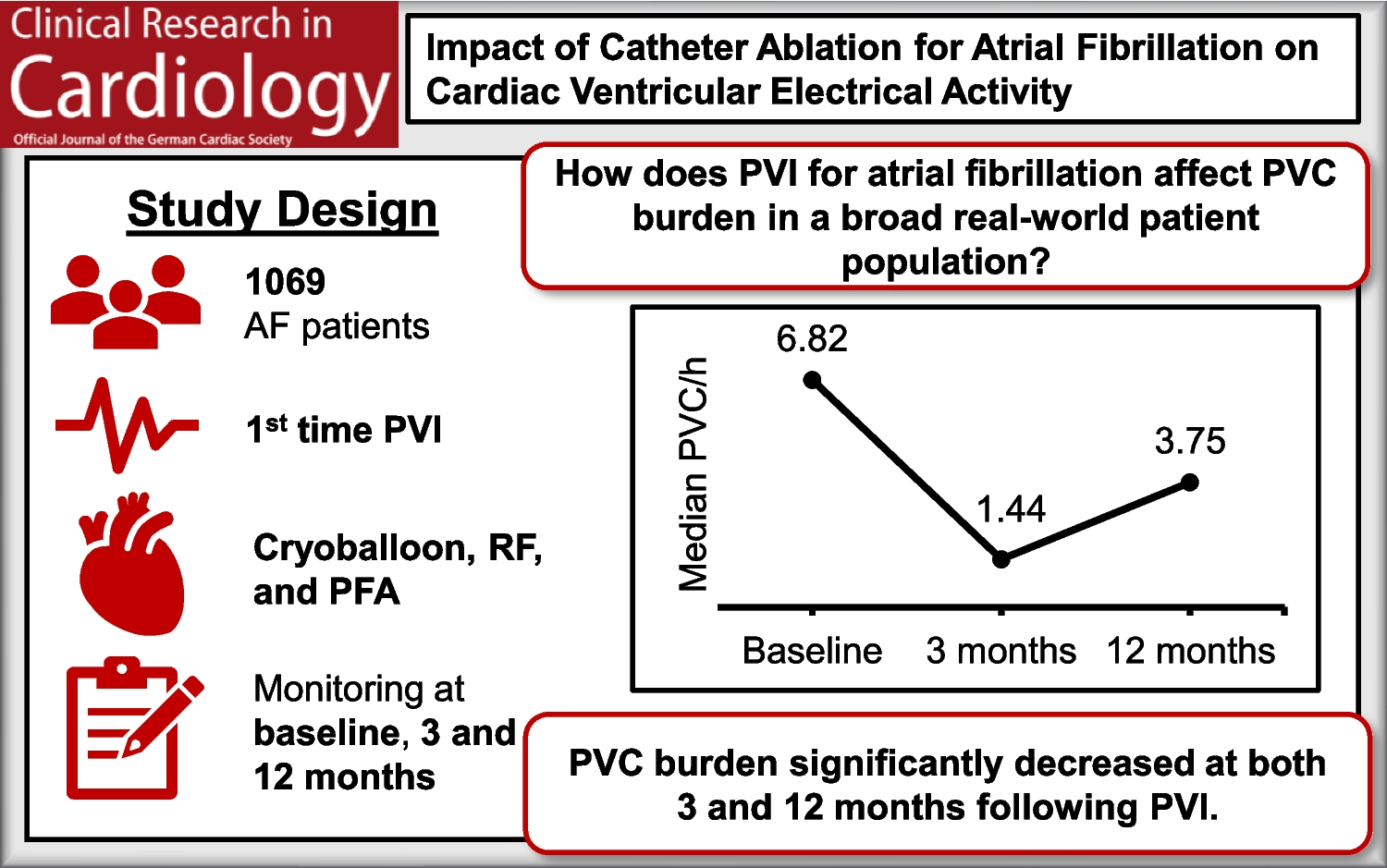
This study demonstrates a significant reduction in PVC burden following PVI, observed at both 3- and 12-month post-ablation. Furthermore, PVC burden was not significantly associated with AF recurrence or the ablation energy source used. Notably, diabetes mellitus and reduced LVEF were independently associated with a high PVC burden at 12 months post-PVI.
Initial studies investigating changes in PVC burden following PVI suggested a potential increase in PVCs post-ablation. For instance, Patel et al. (2014) reported in a prospective study of 53 patients that 11% exhibited elevated outflow tract PVCs, defined as > 3 PVCs per minute or > 30 continuous ventricular beats, within 24 h post-ablation. In 5 of 6 affected patients, this resolved spontaneously [8]. Similarly, Wu et al. (2016) observed an increased PVC burden (≥ 1000 PVCs/24 h) in 4.4% patients within the first months following AF ablation [15]. Jungen et al. (2017) also described a significant rise in PVC in 6 out of 111 patients post-PVI [9]. More recently, Whang et al. (2025) reported a 37.5% incidence of post-ablation PVCs, defined as one or more PVCs within 180 days [16].
In contrast, Choy et al. (2024) found no significant change in PVC burden after 6 months post-PVI compared to baseline, suggesting that earlier studies may have been limited by selection bias—specifically, the inclusion of patients with low baseline and high postprocedural PVC counts. Notably, Choy et al. excluded patients treated with class I or III antiarrhythmic drugs [10].
In our study, we observed a significant reduction in PVC burden at both 3 months and 12 months following PVI. A potential explanation for this finding is that the restoration and maintenance of sinus rhythm may reduce the likelihood of ectopic ventricular activity, potentially by decreasing the excitability of ventricular myocardial cells. Supporting this hypothesis, Lee et al. demonstrated that a high PVC burden (≥ 1000 PVCs/24 h) is associated with an increased risk of developing new-onset AF [17]. Furthermore, patients undergoing PVI in our cohort were closely monitored during follow-up, which may have led to beneficial adjustments in cardiovascular medication and the reinforcement of lifestyle modification. These factors could also help explain the partial rebound in PVC burden observed at 12 months, which may reflect the longer interval between follow-up visits.
Most studies investigating the association between PVC burden and AF recurrence have found no significant relationship, including those by Patel et al., Jungen et al., and Choy et al. [8,9,10]. In contrast, Whang et al. reported that patients with any detectable PVCs (≥ 1 PVCs) had a twofold increased risk of AF recurrence [16]. Similarly, Lee et al. demonstrated that patients a moderate-to-high PVC burden (≥ 1000 PVCs/24 h) had a significantly higher risk of developing now-onset AF over a mean follow-up period of 973 days, compared to those with a low PVC burden (< 1000 PVCs/24 h).
In contrast to these findings, our study did not identify a significant association between PVC burden and AF recurrence at any of the evaluated time points. While some previous studies suggest a potential link between increased PVC burden and AF recurrence, our results do not support this relationship. These discrepancies underscore the need for larger, prospective studies to more clearly define the prognostic role of PVCs in the context of AF management.
Previous studies comparing changes in PVC burden across different ablation energy sources have reported no significant difference. Choy et al., who analyzed the same three energy sources (RF 83%, CRYO 12%, PFA 5%), found no significant variation in PVC burden between groups [10]. Similarly, Whang et al. reported comparable findings on newer technologies, including PFA and high-power, short-duration [16].
These findings are consistent with our results, which revealed no statistically significant differences in PVC burden among the three ablation energy sources (CRYO, RF and PFA) at any time point. Although PVC counts were numerically lower in the PFA group at 3 months, this difference did not reach statistical significance and may be attributable to limited sample size or clinical heterogeneity.
PFA has been hypothesized to be more tissue-selective, potentially sparing non-myocardial structures such as cholinergic nerves innervating the ventricles. However, computational modeling studies suggest that PFA may still generate relevant thermal effects during ablation, which could affect adjacent neural tissue [18, 19].
Wu et al. conducted a multivariable logistic regression analysis adjusted for age, sex, AF type, time since AF diagnosis, comorbidities (including hypertension and diabetes mellitus), echocardiographic parameters, serum NT-proBNP levels, leukocyte counts, C-reactive protein levels, and heart rate within one-month post-ablation. Their cohort included 1,053 patients who underwent first-time RF PVI, of which 46 developed new-onset ventricular tachycardia or a PVC burden ≥ 1000/24 h within one month, excluding those with preexisting ventricular arrhythmias. In this analysis, only elevated serum leukocyte counts were independently associated with the occurrence of ventricular arrhythmias [15].
Other studies have examined the occurrence of PVC after PVI without adjusting for covariates in multivariable models. For example, Whang et al. reported significant differences in LVEF (p = 0.003) and left atrial diameter (p = 0.017) between patients with and without PVCs, but found no significant differences in age, sex, hypertension, diabetes mellitus. In contrast, Patel et al. reported no significant differences in any of these variables.
In our study, diabetes mellitus and reduced LVEF emerged as significant independent predictors of elevated PVC burden at 12 months. Diabetes mellitus was associated with a more than fourfold increase in odds, while reduced LVEF was associated with a more than sixfold increase. These findings align with previous research indicating that metabolic and autonomic dysregulation in diabetic patients may promote ventricular arrhythmogenesis [20]. Moreover, prior studies have demonstrated that a higher PVC burden is linked to impaired LVEF, indicating that reduced LVEF may reflect underlying myocardial damage predisposing to PVCs, while frequent PVCs may further exacerbate left ventricular systolic dysfunction [11, 21]. Analysis of PVC morphology and site of origin may provide additional mechanistic insights. However, as these parameters were not part of the predefined study protocol, they were not systematically collected in our retrospective database. Consequently, this represents an interesting area for future dedicated investigations.
We acknowledge several limitations of our study. The retrospective design and lack of a control group limit causal inference regarding changes in PVC burden. Although both automated analysis and manual verification by specialized personnel were performed, misclassification of PAC with aberrant conduction as PVC cannot be completely excluded and represents an additional limitation. In the multivariable logistic regression model, the pronounced class imbalance in the outcome variable, with 5.5% of patients exhibiting PVC > 5%, further reduced the performance of the regression model, which consequently was unable to reliably classify individual patients. These limitations highlight the need for alternative statistical approaches and larger, prospective studies to confirm our findings and to determine whether reductions in PVC burden translate into improved clinical outcomes or symptom relief. Future research should also explore maintenance strategies to sustain early benefits. In addition, the high proportion of missing data restricted inclusion to only 35.5% of the initial cohort for the main regression analysis, introducing risk of attrition and selection bias and reducing statistical power. In this study, we focused on the effect of PVI on PVC burden across the three ablation energy sources examined, while the influence of specific energy protocols and concomitant procedures (e.g., cavotricuspid isthmus ablation or atrioventricular node ablation) on PVC burden warrants further investigation in future studies.

Comments (0)