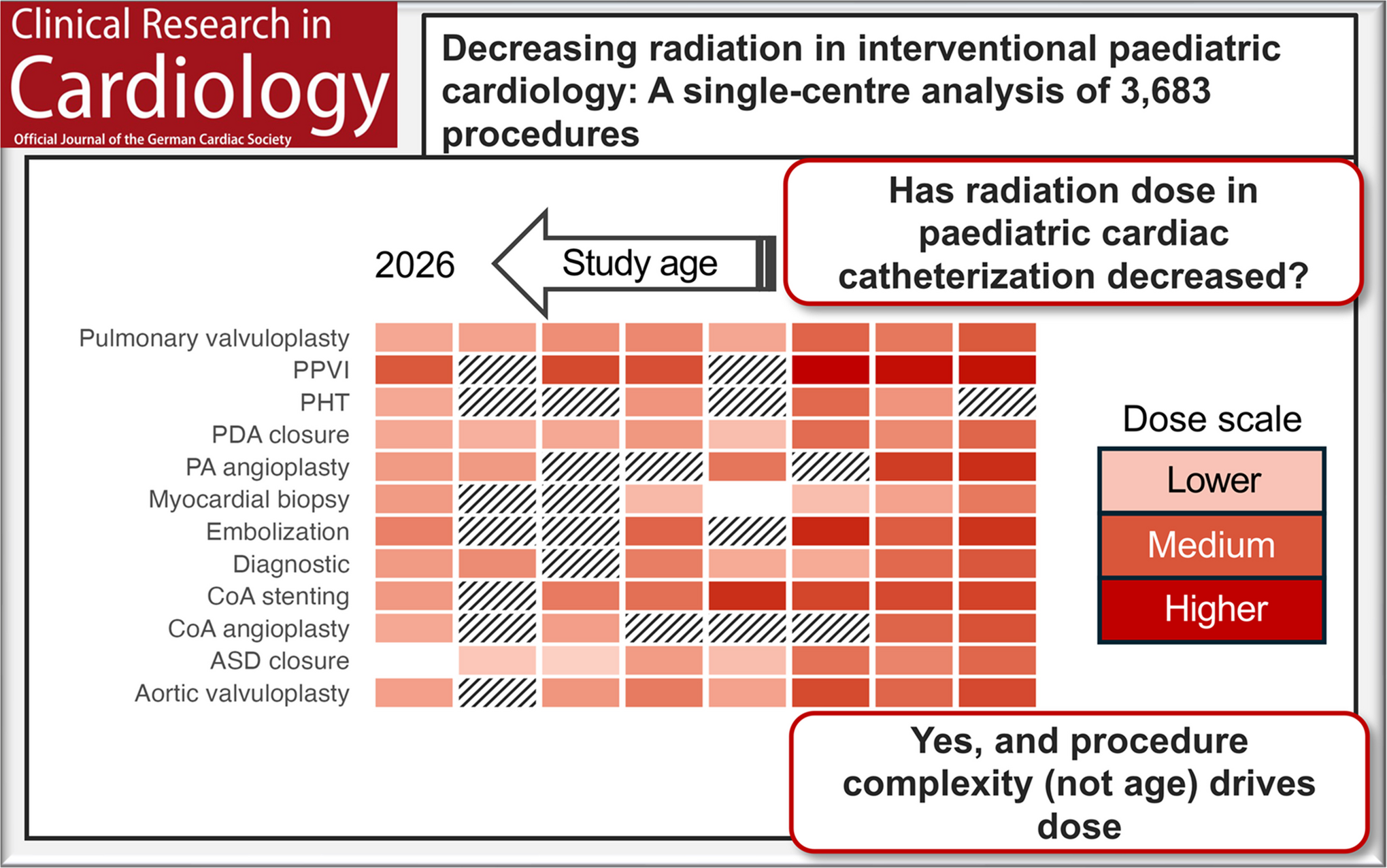
This study analyzed 3,683 pediatric cardiac catheterization procedures performed over a ten-year period, focusing on radiation exposure and ED, and represents by far the largest European single-center study to date.
Compared with published benchmarks around 10 years ago, such as the C3PO study, the medians of DAP/BW in our cohort were approximately 70–80% lower [6].
As previously reported in the literature, the DAP correlated more strongly with body weight than with age [41]. Because this relationship was approximately linear, the established convention of normalizing DAP to body weight appears reasonable. However, reporting of DAP/BW in the literature is highly heterogeneous. DAP/BW is provided in only 57% of published studies, and even when reported, a clear distinction between diagnostic and interventional catheterizations—or between different types of therapeutic interventions—is frequently lacking. As a result, the reported values vary considerably across studies. Moreover, pooled DAP/BW values averaged across all intervention types are strongly influenced by the procedural spectrum of a given center, i.e., its case mix, and therefore reflect institutional practice patterns as much as radiation management strategies.
For these reasons, we consider intervention-specific DAP/BW to be the most meaningful metric for inter-study comparison. In this context, the comparatively low radiation doses observed in our cohort appear consistent with the broader literature: Across centers, a consistent downward trend in radiation dose has been observed over the past decade, a pattern that is also evident—albeit to a lesser degree—at our own institution. During the same period, European centers have generally reported lower DAP/BW values compared with their North American counterparts. This sustained reduction in radiation exposure likely reflects technological advances in imaging systems, continuous refinement of procedural protocols, and growing adherence to radiation safety practices in line with the “As Low As Reasonably Achievable” (ALARA) principle [14]. These trends are in line with the recommendations summarized by Ploussi et al., who reviewed current pediatric interventional practices and dose-reduction strategies under the ALARA framework [5]. For our own center, the trend is explainable with avoiding routine image magnification and preferring stored fluoroscopy over digital acquisition in both planes especially during interventions.
To estimate individual radiation risk, we performed in silico simulations of the ED and derived dose conversion factors between DAP and ED for the fluoroscopy systems used at our center. The resulting factors were very similar, though slightly higher than the conversion factors reported by Dragusin et al. [15]. A plausible explanation is that their estimates were most likely based on ICRP 60 tissue-weighting factors, whereas the organ weighting factor for the breast—highly relevant in cardiac catheterization—has increased by approximately a factor of 2.5 in ICRP 103 [42]. Since the conversion factors for the posterior–anterior and lateral projections differed only minimally, using the mean of both projections is justified, particularly in light of the inherent uncertainties associated with model-based dose calculations. In practice, the higher ED observed for the lateral projection primarily reflects the increased DAP and only to a lesser extent organ weighting factors, in this view.
Body weight itself had only a minor influence on ED. In contrast to the almost proportional influence of body weight on the DAP, doubling body weight only caused an increase in ED by a factor of 1.18 (18%) in contrast to a factor of 2.06 in DAP. In clinical practice, biological radiation risk therefore depends less on patient weight and more on the type and complexity of the intervention. For instance, in our cohort, aortic coarctation angioplasty required a median ED of approximately 1.2 mSv, independent of the child’s age.
Among all interventions, PPVI showed the highest ED, a consistent effect in all reviewed studies. This complex procedure often requires multiple prestents and angled imaging planes, which explains prolonged fluoroscopy time and increased radiation exposure.
At the lower end of the dose spectrum were atrial septal defect (ASD) closure and balloon atrioseptostomy, both of which are—in contrast to the international and national comparison—performed at the study center almost always without fluoroscopy. 72% of all ASD closures and 88% of all atrioseptostomies performed at our center are completely radiation-free. And even the remaining ASD closures are associated with only marginal radiation doses in the context of brief fluoroscopy during wire placement. These findings confirm that radiation-free, echocardiography-guided procedures can achieve a substantial and sustainable reduction in radiation exposure [13].
Estimating the ED is particularly valuable for comparison with other imaging modalities, especially CT. Since CT is used exclusively for diagnostic purposes, such comparisons are most meaningful when limited to diagnostic cardiac catheterizations. In the more recent literature, ED was reported in only six studies, as shown by our structured review [20, 21, 26, 27, 29, 41]; in most of these, it was estimated only as an average across all intervention types. In our study, the median ED for diagnostic catheterization was 1.8 mSv, which is considerably lower than values reported in earlier studies (3.8–10 mSv) [43] but slightly higher than those achieved with modern cardiac CT protocols. For recent CT techniques using prospective electrocardiogram (ECG)-gating, radiation doses between 0.2 and 1.0 mSv have been reported, whereas older protocols with retrospective ECG-gating reached up to 10 mSv [44, 45]. Thus, diagnostic cardiac catheterization currently is more dose-intensive than CT and should primarily be reserved for cases in which additional hemodynamic information is required [46].
Approximately one quarter of children in this cohort underwent more than one catheterization, making cumulative radiation exposure a significant long-term individual risk [25]. Consequently, minimizing radiation doses and promoting radiation-free techniques remain essential. The most effective way to reduce exposure is to eliminate ionizing radiation altogether, as successfully implemented in our center for ASD closure and balloon atrioseptostomy.
This study has several limitations in addition to its retrospective design. While results from single-center studies are only partially generalizable, homogeneous datasets from individual institutions can serve as valuable, up-to-date benchmarks and can easily be incorporated into future meta-analyses. Second, the individual impact of specific interventionalists on radiation exposure could not be assessed, as this information was not documented. Part of the observed dose reduction over the study period may therefore be attributable to a learning-curve effect among operators who remained constant throughout the study. Third, estimation of the ED was based on model calculations assuming strictly orthogonal beam projections (posterior–anterior and lateral), which only approximate real-world imaging conditions and represent a potential source of uncertainty in dose modeling. However, we were able to demonstrate that the projection used contributes to the estimated ED primarily through its associated higher DAP, rather than through differences in organ weighting factors.
In summary, this large European single-center analysis demonstrates that radiation exposure in pediatric cardiac catheterization procedures today represents only a fraction of the levels reported in the literature a decade ago. Effective dose is predominantly determined by procedural complexity, whereas patient weight and age contribute only to a lesser extent. Given the continuously increasing life expectancy of this patient population, strategies aimed at further reducing radiation exposure and developing radiation-free imaging alternatives should be consistently advanced.

Comments (0)