
Remember me
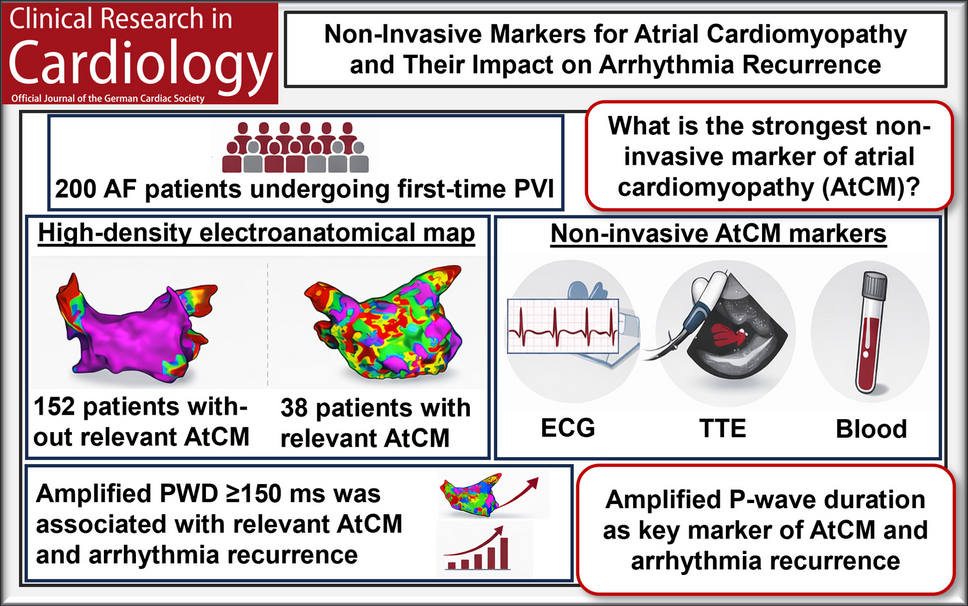
In this comprehensive analysis of patients undergoing first-time AF ablation, we evaluated the clinical utility of non-invasive AtCM markers to identify advanced atrial disease and predict rhythm outcomes. Several key findings emerge: First, among a broad panel of ECG-, TTE-, and blood-based parameters, amplified PWD and P-wave amplitude in lead I demonstrated the strongest and most consistent associations with invasively quantified LA-LVS, which served as the reference standard for AtCM (Fig. 4). Second, amplified PWD was the only non-invasive AtCM marker that was not only associated with advanced atrial disease but also independently predicted arrhythmia recurrence following first-time PVI.
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Multimodal characterization of AtCM.
Representative examples of patients without AtCM (left panel, green frame) and with relevant AtCM (right panel, red frame) integrating invasive electroanatomical mapping (EAM), electrocardiography (ECG), transthoracic echocardiography (TTE), and blood-based biomarkers. (a) Electroanatomical voltage maps of the left atrium demonstrating preserved atrial voltage in patients without AtCM and extensive left-atrial low-voltage substrate (LA-LVS) in patients with relevant AtCM. (b) ECG analysis illustrating shorter amplified P-wave duration (APWD), higher P-wave amplitude in lead I and normal P-wave axis in patients without AtCM, compared with prolonged APWD, reduced P-wave amplitude in lead I and pathological P-wave axis in patients with relevant AtCM. (c) TTE showing normal left atrial volume index (LAVI) and absence of relevant mitral regurgitation in patients without AtCM versus left atrial enlargement and relevant mitral regurgitation in patients with relevant AtCM. (d) High-sensitivity troponin T as a blood-based biomarker was within the normal range in patients without AtCM and elevated in patients with relevant AtCM
EAM for AtCM quantificationThe concept of AtCM describes atrial remodeling beyond the mere presence of AF, encompassing structural, electrical, and functional alterations of the atrial myocardium [8, 9, 13]. In this context, LA-LVS identified by EAM have emerged as the most established surrogate of AtCM and have been consistently linked to adverse ablation outcomes [10, 13]. The definition of LA-LVS based on a bipolar voltage threshold of < 0.5 mV represents a simplified but widely used approach for characterizing atrial structural remodeling and is therefore also adopted in the current AtCM consensus statement [8]. However, histological validation studies have demonstrated that normal bipolar voltage varies across different atrial regions and that atrial structural remodeling in patients with AF is not solely characterized by localized fibrosis but rather represents a diffuse process involving fibrosis, increased intercellular space, myofibrillar loss, and reduced cardiomyocyte density [4, 22, 23]. Consequently, it may not be appropriate to assume a single universal LA-LVS cut-off for accurately quantifying the extent of AtCM [4]. Nevertheless, while alternative approaches such as individualized voltage thresholds or analysis of global voltage distributions may provide additional insights, the commonly used threshold of < 0.5 mV remains a pragmatic and widely accepted definition for clinically relevant atrial substrate [4, 8, 22]. This threshold has therefore been applied in many studies investigating AtCM and AF ablation outcomes and was also used in our study to ensure comparability with previous literature and to facilitate interpretation within established AtCM staging frameworks.
Another important aspect relates to technical factors that may influence voltage mapping. Several studies have demonstrated that bipolar electrogram amplitudes can vary depending on the activation rate, the orientation of the activation wavefront relative to the electrode pair, and the inter-electrode spacing of the mapping catheter, potentially leading to differences in the detected extent of LA-LVS [24,25,26]. In our study, coronary sinus pacing during EAM was performed in 81 patients (40.5%), while in the remaining 119 patients mapping was conducted during sinus rhythm. A high-density multipolar mapping catheter with small inter-electrode spacing was used in all patients, which likely mitigates wavefront direction–dependent effects by sampling activation from multiple orientations and thereby improves the robustness of voltage characterization [27]. In addition, coronary sinus pacing was performed at cycle lengths between 600 and 700 ms, which approximate the intrinsic sinus cycle length in most patients and bipolar voltage amplitudes are therefore likely to remain largely comparable between sinus rhythm and coronary sinus pacing [24].
Yamaguchi et al. defined four stages of LA-LVS and demonstrated that patients with relevant LA-LVS (≥ 20% of the left atrial surface area) exhibited a significantly increased recurrence rate following PVI which is consistent with the findings in our study [10]. However, the invasive nature of EAM limits its applicability for preprocedural risk stratification [8, 9].
Non-invasive ECG markers as surrogates of AtCMOur findings demonstrate that amplified PWD closely reflects the extent of LA-LVS. This observation aligns with prior reports linking prolonged PWD to interatrial conduction abnormalities in patients with AtCM [12, 13]. By enhancing low-amplitude terminal P-wave components, amplified ECG analysis appears particularly sensitive to advanced atrial remodeling and may therefore outperform standard non-amplified PWD in detecting conduction delay [12]. This mechanism may also explain observations from earlier studies in which both prolonged and paradoxically short non-amplified PWD were associated with an increased risk of AF and stroke [28, 29]. In individuals with advanced AtCM, delayed terminal atrial activation may remain undetected on standard ECG recordings, resulting in an apparently short PWD despite prolonged overall atrial conduction. Signal amplification enables visualization of these terminal components and thus provides a more accurate estimate of total atrial activation time. Consistent with this concept, amplified PWD showed a strong correlation with IAAT in our cohort, supporting its pathophysiological relevance as a marker of global atrial conduction delay. Moreover, the predefined cut-off of ≥ 150 ms was associated with a more than 11-fold increased risk of relevant AtCM in multivariable regression analysis and emerged as the only AtCM marker significantly associated with arrhythmia recurrence, corresponding to an approximately twofold increased risk after PVI [12].
In parallel, reduced P-wave amplitude in lead I was an independent marker of relevant AtCM [11]. Decreased atrial P-wave amplitude likely reflects loss of viable atrial myocardium, altered atrial activation vectors, or electrical uncoupling due to fibrotic remodeling [11, 14]. While P-wave amplitude has received less attention than PWD, our results suggest that it captures complementary information on atrial myocardial integrity and may therefore enhance non-invasive substrate characterization. However, the predefined cut-off of ≤ 0.1 mV was not significantly associated with relevant AtCM in our cohort, and, in contrast to amplified PWD, P-wave amplitude did not predict arrhythmia recurrence following PVI.
Comparison with TTE and blood-based biomarkersElevated LAVI, reduced LV-EF, relevant mitral regurgitation, and increased high-sensitivity troponin T levels were all associated with relevant AtCM in univariable analyses, reflecting the close interplay between atrial enlargement, ventricular function, and myocardial injury [8, 9, 16]. However, none of these parameters retained independent significance after adjustment for ECG-derived markers and other clinical risk factors.
These findings suggest that while these TTE and blood-based biomarkers reflect global cardiovascular disease burden, ECG markers may more directly capture atrial-specific electrical remodeling, particularly compared with structural markers of atrial dilatation alone. However, left atrial strain analysis, which represents a more specific marker of AtCM by directly quantifying atrial mechanical function, was not available in the present study [5].
Sex-specific aspects of AtCMFemale sex emerged as a strong independent predictor of relevant AtCM and female patients exhibited a substantially higher burden of LA-LVS compared with men (15.9% versus 3.8%, p < 0.001) in the present study. This finding is consistent with previous reports demonstrating more advanced AtCM, including more extensive LA-LVS, lower global atrial voltage, slower conduction velocity and a higher proportion of complex fractionated signals, as well as worse ablation outcomes in women despite smaller atrial dimensions [30,31,32]. Potential underlying mechanisms include hormonal influences on fibrotic remodelling and later referral for catheter ablation procedures [33, 34]. However, the interpretation of sex-related differences in LA-LVS is complex. Recent studies combining high-density EAM with atrial biopsy have demonstrated that women exhibit lower atrial voltage even in the absence of AF, which may partly reflect intrinsic differences in atrial myocardial architecture, including smaller cardiomyocyte size and lower atrial mass [35]. Consequently, the use of uniform bipolar voltage thresholds could potentially lead to differences in the detected extent of LA-LVS between sexes. Although the present study was not designed to investigate mechanistic sex differences, our findings underscore the importance of incorporating sex-specific considerations into AtCM assessment and risk stratification. Notably, despite a greater LA-LVS extent, arrhythmia recurrence rates did not differ significantly between men and women in our cohort. Therefore, sex-specific voltage thresholds for defining LA-LVS may deserve consideration in future studies.
Clinical implicationsTo the best of our knowledge, this is the first study to systematically compare non-invasive AtCM markers in a large cohort of patients with AF using comprehensive EAM data as a reference standard for AtCM assessment (Fig. 4). Our findings align with recent consensus statements emphasizing electrical and structural atrial remodelling as core components of AtCM and have several clinically relevant implications [8, 9].
First, ECG-derived markers, most notably amplified PWD, enable non-invasive identification of patients with advanced AtCM prior to ablation. This may improve procedural planning, for example by supporting the decision to perform PVI in conjunction with EAM to identify and treat additional extra-pulmonary vein substrate, as was applied in patients with more extensive LA-LVS in the present cohort. Second, the association between amplified PWD and arrhythmia recurrence suggests that ECG-based AtCM markers capture atrial substrate characteristics that extend beyond pulmonary vein triggers and contribute to ablation failure as shown in our cohort. This information may be valuable for pre-procedural risk communication and expectation management prior to PVI. Moreover, accumulating evidence indicates that AtCM is independently associated with an increased risk of thromboembolic events, even in the absence of documented AF [1, 6, 7]. Non-invasive markers of AtCM may therefore not only support rhythm-related risk stratification but could also contribute to improved assessment of stroke risk. However, this potential application requires validation in large, prospective outcome studies.
Importantly, surface ECG analysis appears particularly well suited for screening purposes. ECGs are inexpensive, ubiquitously available, and easily repeatable, and their interpretation does not rely on advanced imaging infrastructure or specialized TTE expertise. Signal amplification can be readily implemented using several standard digital ECG systems without the need for additional hardware, suggesting that amplified PWD may represent a simple and accessible tool for non-invasive identification of advanced atrial disease in clinical practice. Nevertheless, automated algorithms for amplified PWD measurement will be required to enable scalable implementation in routine practice. With such developments, ECG-based assessment of AtCM could represent a pragmatic first-line screening tool, particularly in settings with limited access to advanced imaging modalities.
LimitationsSeveral limitations merit consideration. First, this was a single-center, retrospective study, which may limit generalizability. Second, although high-density EAM was performed using standardized protocols, voltage thresholds and mapping techniques remain subject to methodological variability. Nevertheless, a widely used bipolar LA-LVS cut-off (< 0.5 mV) was applied, and mapping quality was ensured by high point density and contact verification, supporting the robustness of LA-LVS quantification.
Third, tissue proximity index during EAM was not used in all procedures. In these cases, LA-LVS was verified using a contact force–sensing ablation catheter to confirm adequate PentaRay catheter–tissue contact. While larger electrode size of the ablation catheter limits spatial resolution compared with the multipolar mapping catheter, this verification step was primarily implemented to exclude false-positive LA-LVS due to insufficient tissue contact rather than to replace high-density mapping. Moreover, the majority of patients without tissue proximity index were classified as AtCM stage I, where the absence of substantial LA-LVS makes misclassification due to insufficient tissue contact unlikely. Fourth, arrhythmia recurrence was assessed using intermittent rhythm monitoring, which may underestimate asymptomatic recurrences. Nevertheless, this approach reflects routine clinical follow-up in many centers and is unlikely to differentially affect comparisons between marker-defined subgroups. Fifth, while the analysis focused on established ECG-derived parameters, more advanced signal-processing techniques or machine-learning–based approaches were not evaluated. Finally, inclusion required the availability of a baseline ECG recorded in sinus rhythm to enable AtCM assessment, which may have introduced selection bias. However, this criterion was necessary to ensure reliable AtCM marker analysis.
Comments (0)