
Remember me

Early-infantile DEEs include Ohtahara syndrome and early myoclonic encephalopathy, which were previously considered two distinct entities, but whose designations were abandoned in the latest ILAE position statement on the different epilepsy syndromes [4]. The etiologies are therefore highly diverse, most commonly being genetic, structural, and/or metabolic. By definition, seizure onset must be within the first 3 months of life, and abnormalities on neurological examination (of tone, posture, or movement), a developmental disorder (which may still be difficult to detect), frequent seizures, and pharmacoresistance must be present. The interictal electroencephalogram (EEG) is highly abnormal, showing a burst-suppression pattern, a discontinuous pattern, diffuse slowing, or multifocal discharges [4]. Further diagnostic tests such as cerebral imaging and genetic and metabolic analyses enable an accurate etiologic classification in up to 80% of affected neonates and infants ([6]; Table 1).
Table 1 Early infantile developmental and epileptic encephalopathy (DEE)Epidemiology and clinical presentationWith an incidence of 10/100,000 live births, early-infantile DEE is rare. The first seizures occur within the first 3 months of life. These children do not become seizure-free with conventional antiseizure therapies and, as mentioned earlier, show abnormalities on neurological examination and in their development [5].
Precision medicine now allows certain gene variant-specific therapies to be used, such as sodium channel blockers, often in high doses, for KCNQ2 (and KCNQ3, both loss of function), SCN2A, and SCN8A (gain of function) and quinidine for KCNT1 [7,8,9,10].
On the other hand, epilepsy surgery should always be discussed if the prerequisites are met.
Seizures, electroencephalogram patterns, and movement disordersSeizure semiologies in the context of early-infantile DEEs include tonic, myoclonic, and epileptic spasms, as well as sequential seizures (i.e., multiple semiologies in succession within a seizure, typically KCNQ2 with tonic onset).
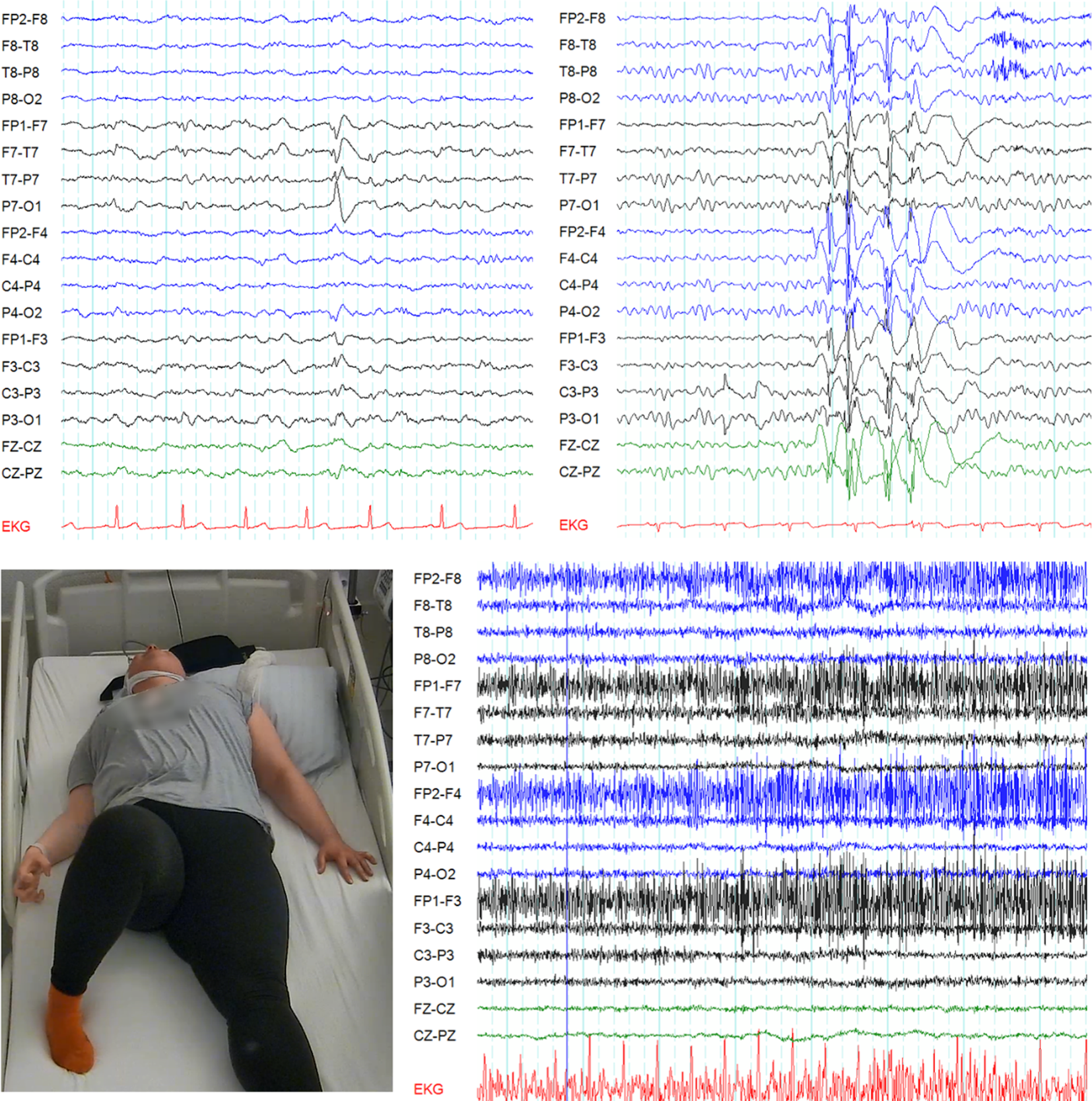
Various interictal patterns are possible, but typically a burst-suppression pattern is seen, i.e., high-voltage burst activity (150–300 µV) consisting of spikes, sharp waves, sharp and slow waves alternating with a suppressed phase (amplitude < 5 µV). The duration of the suppressed phase is also influenced by the administration of barbiturates, for example, or by the child’s state of alertness. However, discontinuous patterns, multifocal spikes, sharp waves, sharp and slow waves, and diffuse slowing are also possible (examples in Figs. 2, 3, 4, 5, 6, 7, and 8).
Fig. 2 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Ictal and interictal electroencephalogram (age 1 week, amplitude 15 µV): burst-suppression pattern in metabolic early-infantile developmental and epileptic encephalopathy due to a cholesterol metabolism disorder. Clinical presentation: erratic myoclonus during bursts (first half of the image), tonic seizures, and movement disorders (not shown)
Fig. 3 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Interictal electroencephalogram (age 2 days, amplitude 7 µV): discontinuous background in glycine encephalopathy. Clinical presentation: focal seizures
Fig. 4 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Ictal electroencephalogram (age 3 days, amplitude 7 µV): sequential seizure with a a tonic phase, b a clonic phase (first half of the image, bilateral spikes and waves) followed by another tonic phase (second half of the page, bilateral flattening of amplitude and rapid activity), and c an autonomic phase with apnea (note absence of abdominal movement in the second half of the image) due to a KCNQ2 variant
Fig. 5 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Interictal electroencephalogram (age 6 weeks, amplitude 10 µV): increased beta activity due to PAFAH1B1 (LIS) variant. Clinical presentation: focal clonic seizures and behavioral arrest
Fig. 6 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Interictal electroencephalogram (age 4 months, amplitude 10 µV): deterioration of the EEG with hypsarrhythmia, partly fragmented. Clinical presentation: spasms
Fig. 7 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Interictal electroencephalogram (age 4 months, amplitude 10 µV): diffuse slowing with superimposed sharp waves and sharp-and-slow wave complexes in the right hemisphere due to a CDKL5 variant. Clinical presentation: tonic seizures
Fig. 8 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.Interictal electroencephalogram (age 6 weeks, amplitude 7 µV): discontinuous background, intermittent burst-suppression (not shown), and multifocal spikes due to a compound heterozygous RARS2 variant. Clinical presentation: focal clonic seizures, lactic acidosis, hypoglycemia
In addition to epileptic seizures, neonates and infants with early-infantile DEE also exhibit movement disorders with chorea, non-epileptic myoclonus, dystonia, and tremor [5].
Comments (0)