
Remember me
This retrospective study was conducted at a single tertiary center (Seoul National University Hospital, Republic of Korea), and the requirement for written informed consent was waived (IRB No: 2307-207-1457).
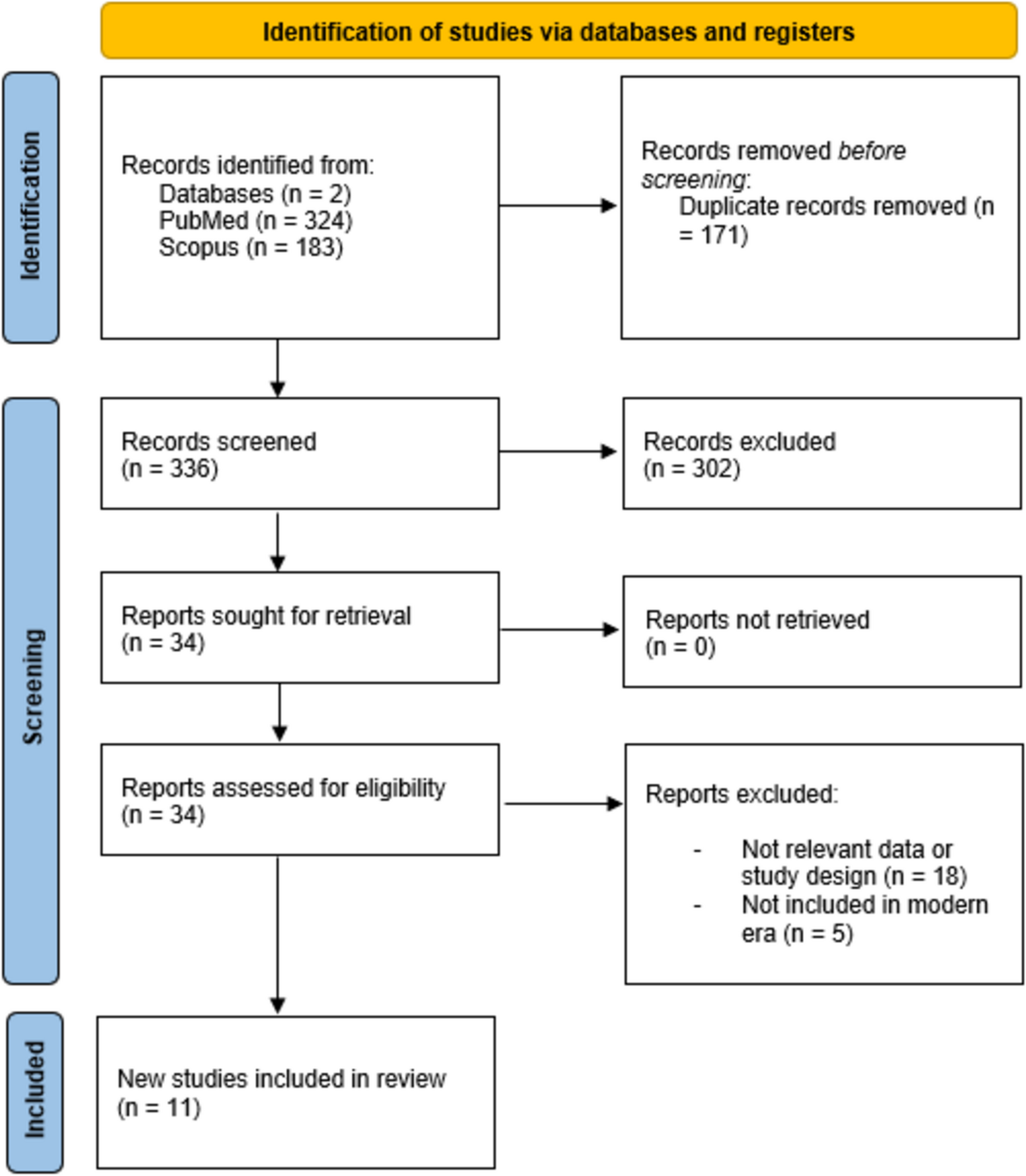
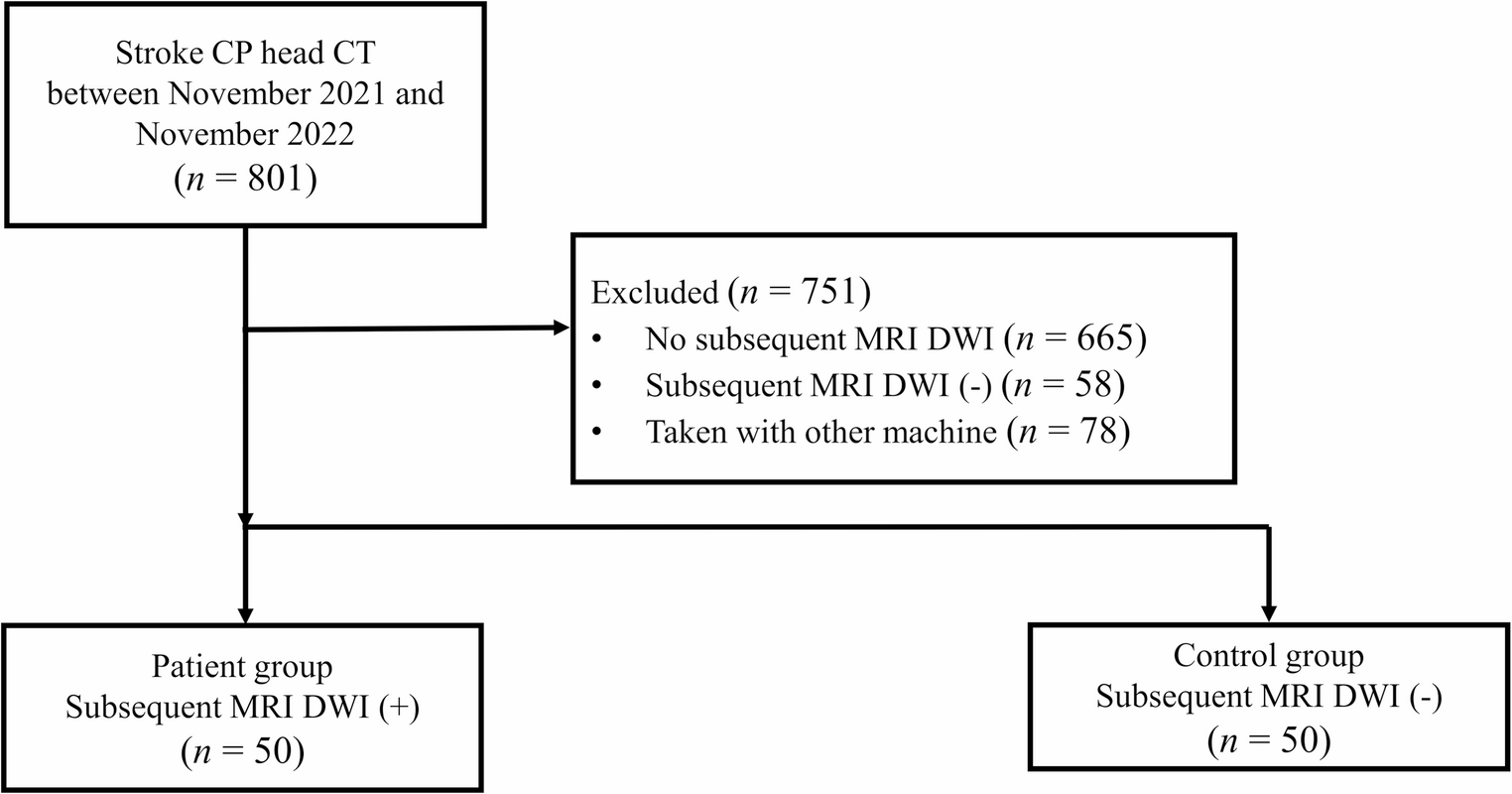
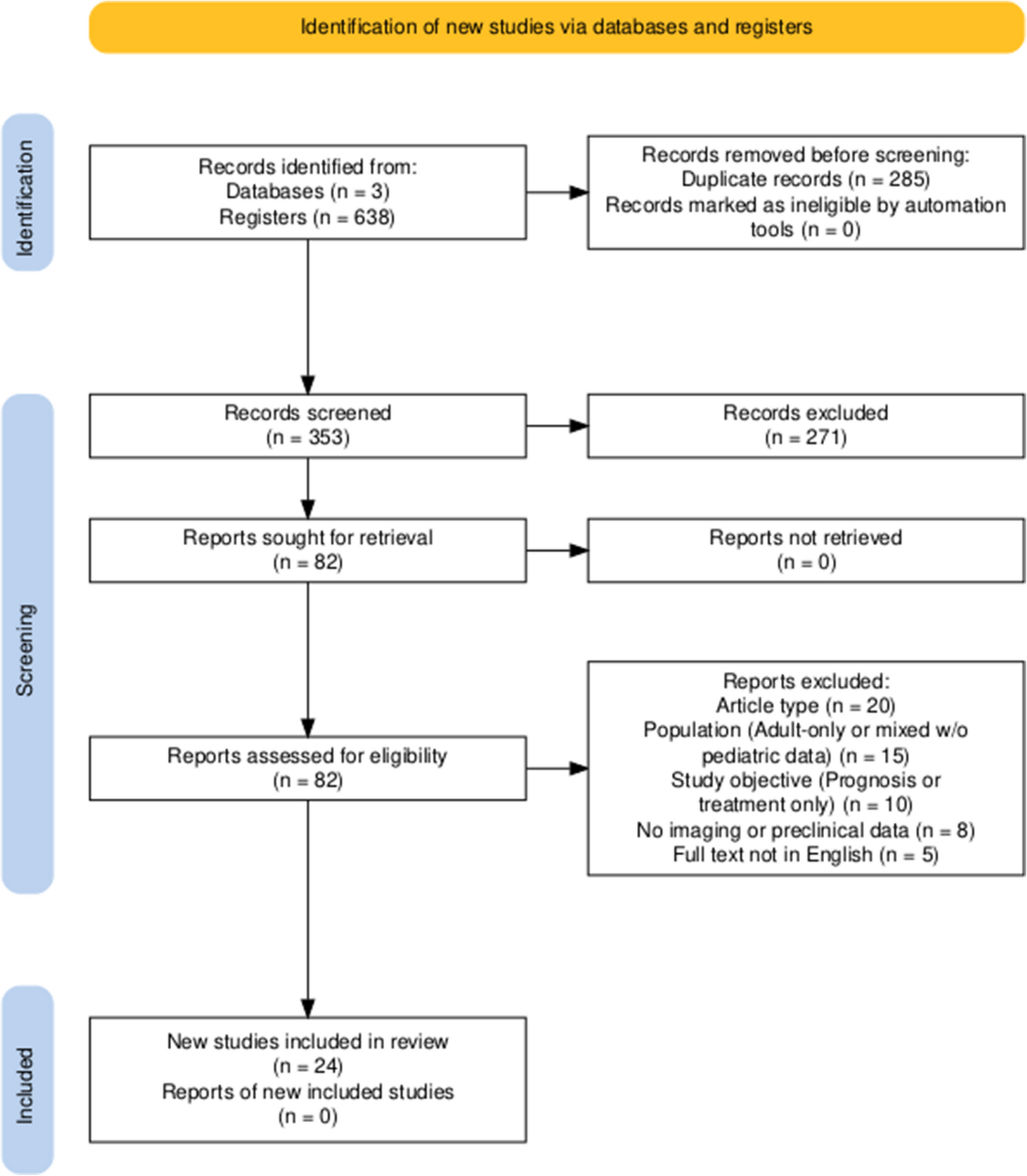
One radiologist searched the radiology database of our institution from November 2021 to November 2022 to identify patients who met the study eligibility criteria. The inclusion criteria were as follows: (a) patients aged 19 years or older who presented to our institution’s emergency department with suspected acute stroke; (b) patients who underwent noncontrast head CT on a dedicated CT scanner with wide-detector capability for whole-brain perfusion imaging as part of a stroke critical pathway; and (c) patients who underwent subsequent MRI with diffusion-weighted imaging (DWI) within 1 day (Fig. 1). Patients with substantial brain lesions other than ischemic stroke (stroke mimickers, e.g., hemorrhage or tumor) were excluded. The patient group was composed of 50 consecutive patients confirmed to have acute ischemic strokes on the basis of subsequent DWI. In addition, the control group consisted of the first 50 consecutive patients without acute ischemic lesion on DWI. Finally, 100 patients were included in this study. Patient characteristics, including sex, age, last recorded normal time and first recorded abnormal time, were collected from electronic medical records.
Fig. 1
Flowchart of the inclusion and exclusion criteria for the main study population CP: Critical pathway; MRI: Magnetic resonance imaging; DWI: Diffusion weighted image
CT acquisition and image reconstructionAll patients underwent noncontrast head CT scans on a 320-channel CT scanner (Aquilion ONE, Canon Medical Systems, Tochigi, Japan). The scan parameters were as follows: tube voltage, 120 kVP; effective tube current time product, 240 mAs; beam collimation, 0.5 × 40 mm; volume computed tomography dose index (CTDIvol), 48.11 mGy; field of view, 240 × 240 mm; and matrix 512 × 512.
All CT datasets were reconstructed using vendor-provided hybrid IR (adaptive iterative dose reduction, AIDR) images with brain kernel (FC68) and vendor-agnostic DLR (ClariCT.AI, ClariPi, South Korea) images. The DLR model is a vendor-agnostic U-net–based CNN denoising algorithm trained on > 1 million CT images generated using synthetic sinogram-based low-dose simulation across diverse vendors, scanners, and reconstruction settings. Its performance has been validated in multiple clinical studies of body and pediatric imaging [14,15,16]. The reconstructed images had a slice thickness of 3 mm and the same field of view. All the images were successfully processed. The representative pair images of normal head CT reconstructed by DLR and IR are shown in Fig. 2.
Fig. 2
Example of two differently reconstructed normal head images from the same CT scan. Compared to vendor-provided hybrid iterative reconstruction image (adaptive iterative dose reduction, AIDR, Canon Medical Systems) (a), deep-learning reconstruction image (ClariCT.AI, ClariPi) exhibited reduced noise and improved delineation of gray-white matter boundaries (b)
Observer study and quantitative measurementsThe image quality of the 200 reconstructed noncontrast head CT images was evaluated by two radiology residents (readers 1 and 2, third and second years of training, respectively) and two neuroradiologists (readers 3 and 4, with 12 and 10 years of experience in neuroradiology, respectively). All observers were blinded to the patient information and reconstruction parameters during the evaluation process. The observers could adjust the window width and window level as they deemed appropriate. The observers were blinded to the reconstruction techniques and diagnosis. The images were presented to the observers in randomized order.
Subjective image quality was evaluated using a 5-point Likert scale, assessing both overall image quality score and GM/WM differentiation score. For overall image quality, the scores were as follows. Score 1, nondiagnostic; 2, poor image quality, insufficient for the evaluation of subtle pathology; 3, moderate image quality, sufficient for soft tissue evaluation; 4, good image quality, equal to the current standard; 5, excellent image quality, superior to the current standard. For GM/WM differentiation, the scores were as follows. Score 1, poor GM/WM differentiation, impaired diagnostic quality; 2, reduced GM/WM differentiation, reduced diagnostic quality; 3, acceptable GM/WM differentiation, lower than the current standard; 4, average GM/WM differentiation, equal to the current standard; and 5, better GM/WM differentiation than the current standard. Additionally, the degree of image noise and artifacts was evaluated using a 3-point scale (Supplementary Tables 1 and 2).
Diagnostic performance was assessed through acute ischemic lesion conspicuity using a 5-point scale, and the score parameters were as follows: 1, no focal lesion; 2, low probability (> 5% and < 25%); 3, intermediate probability (> 25% and < 75%); 4, high probability (> 75% and < 90%); and 5, definite (> 90%) (Supplementary Table 3).
Statistical analysisFor qualitative image quality assessment, mean scores for overall image quality, GM/WM differentiation, image noise and degree of artifacts were calculated for each reader and averaged across all the readers. The mean values were compared using the Wilcoxon signed-rank test. Interobserver agreement was assessed using Gwet’s AC2 with quadratic weights [17]. For diagnostic performance assessment, the mean scores of ischemic lesion conspicuity for each reader were calculated and compared using the Wilcoxon signed-rank test. Single-reader receiver operating characteristic (ROC) curve analyses were conducted for each reader, and multireader, multicase ROC curve analysis with random case and random reader models was performed for the reader subgroups according to the readers’ experience (residents vs. neuroradiologists) [18, 19]. The significance level was set at 0.05. All statistical analyses were performed using R (version 4.2.3; R Core Team, 2023); the “MRMCaov” package was used for multireader ROC analysis, and the “irrCAC” package was utilized for interobserver agreement.
Comments (0)