We developed an algorithm that automated PC image processing with measures for each key analysis step and had image analysts manually process the same images in a blinded fashion to automated output. Because pediatric PC images are generally of lower quality and more challenging to analyze than adult PC images [12], we evaluated the algorithm on both pediatric and adult PC images. Overall manual and algorithm performance were similar in pediatric and adult images, with better overall algorithm reliability in pediatric images.
Manual processing of MR images is prone to both inter- and intra-operator variability [27], indicating a need for automated approaches with greater consistency. The automated algorithm and manual processing performed similarly for vessel segmentation for both pediatric and adult images. As expected, segmentation results from two analysts were less precise than one analyst performing segmentation twice, and as expected, both were inferior to automation which produces identical results. Automated vessel unaliasing was superior to the manual approach that introduced errors from overestimation and incorrect voxel selection. The algorithm and manual processing also performed similarly for vessel identification for both pediatric and adult images. Overall CBF calculations had high reliability across the automated and manual methods. However, when calculating CBF from ICA and VA flows, the user should check for errors in segmentation, unaliasing, identification, and provide manual correction as needed. For lower quality PC images, ICAs and VAs are harder to segment for both image analysts and the algorithm. Differences of just a few voxels in segmentation can cause errors in unaliasing or flow calculation, leading to incorrectly identified vessels.
All methods had lower reliability in CBF calculations for pediatric participants with neurological tumors than their matched cohort. Images from children with neurological tumors may be more difficult to process, highlighting the need for a precise automated method.
ASL image acquisitions were improved by adopting standardized guidelines [11]. We can also improve PC image acquisitions by creating similar standardized guidelines. PC images vary as differing protocols are implemented by MR technologists at time of acquisition. Efforts to estimate and minimize variations from differing MR vendors, field strengths, gradient strength, gradient slew rate, or coils would improve the reliability of CBF measures between sites and across time at a single site.
The successful development and validation of an automated algorithm for processing of PC images has important implications for measuring CBF in research and eventual clinical use. Algorithmic CBF measures provide potential for increased consistency over time, avoiding human bias in CBF estimation from separate individuals performing manual analysis. Longitudinal studies and those with multiple data acquisition sites would benefit especially in this regard. Acquisition times for PC images are short (less than 2 min) and, when combined with our automated processing algorithm, can be used to validate CBF measures obtained using other methods (e.g. ASL).
Limitations
Our participants were from 2 different cohorts consisting of young children and adults. We therefore did not evaluate algorithm performance in adolescents. However, we expect the performance of our algorithm to improve in adolescent populations because PC acquisitions are more challenging in young children due to their smaller arteries, lower blood flow, and increased likelihood of movement while scanning. Additionally, some children were imaged under anesthesia, which may lower CBF. Since PC imaging involves calculation of blood flow via voxel sampling of blood velocity within vessel lumens, lower CBF in anesthetized children diminishes image quality. As a result, our pediatric PC images are generally of lower quality compared to those of adults. We included only a small number of children with tumors, and they did not receive ASL imaging, however the main focus of our work was improving PC processing.
The 2 cohorts were imaged on different MR scanners and with different imaging parameters. However, the area of focus for our study was the processing performance on pediatric and adult images. Because scanner and cohort ages were perfectly confounded, we are not able to distinguish differences in processing pediatric and adult images from differences in processing images from different scanners. We cannot rule out that our algorithm’s performance may differ by either scanner acquisition or age. Nevertheless, these differences in image acquisition parameters and quality are useful for validating the robustness of the automated algorithm. If the images were of poor image quality because they did not consider age-dependent factors, then acquisitions with higher image quality would be expected to yield noninferior or superior algorithm performance.
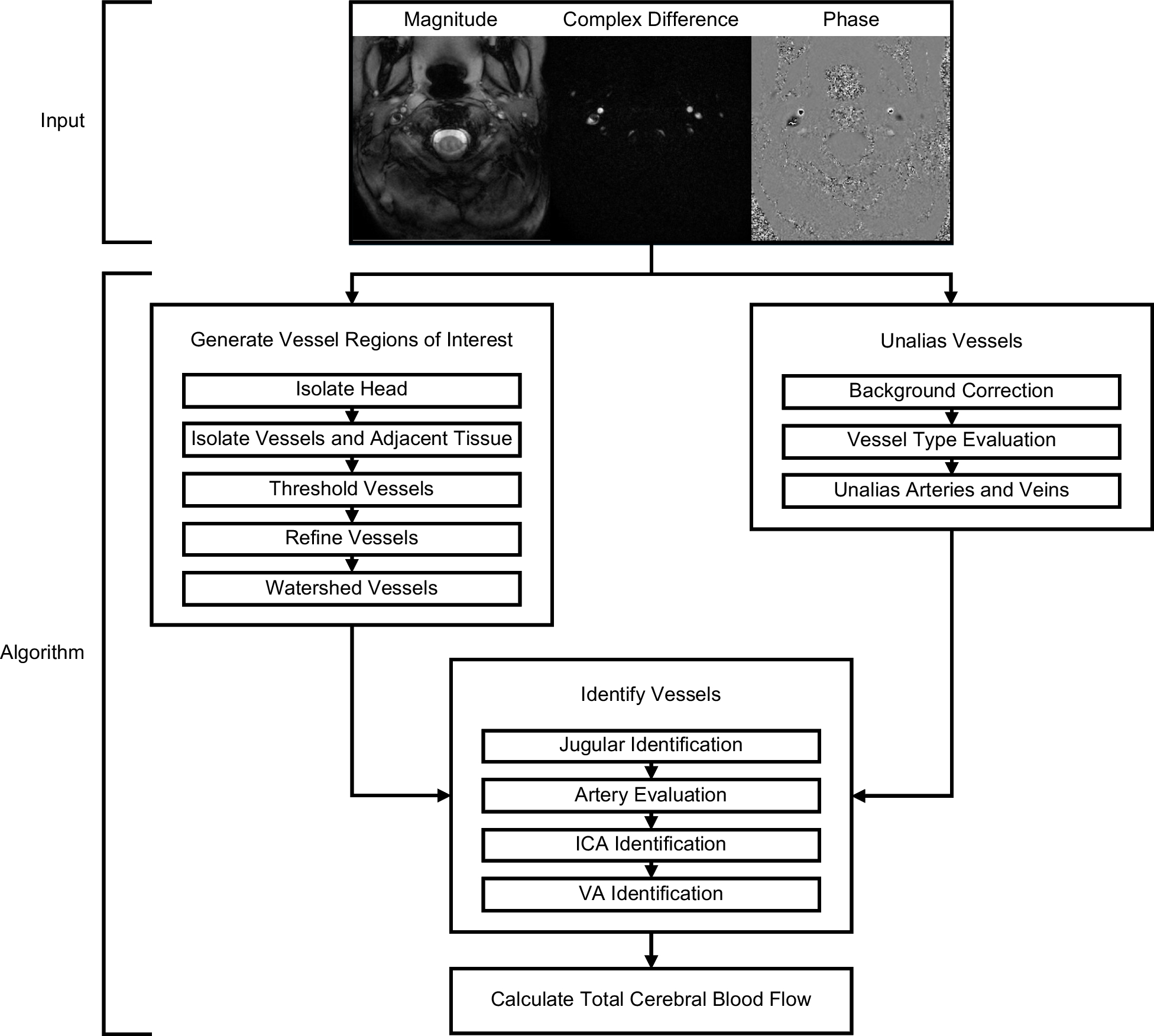
In addition, incorrect placement of the imaging slice may result in capturing oblique ICAs and VAs or external carotid arteries that would complicate segmentation or identification, respectively. For these suboptimal cases, the algorithm has the capability for manual correction in segmentation and identification. Mathematical models can also be employed to accurately impute CBF [28]. Not all scanners may provide the 3 images required by the algorithm from Philips and Siemens scanners (magnitude, complex difference, phase). For components such as vessel segmentation, the algorithm could be developed further to explore the use of only magnitude and phase images.
Common practice involves acquiring dynamic PC images throughout the cardiac cycle, which enables measurement of flow within the cardiac cycle. However, the PC sequence we analyzed acquired and averaged images, and thus it can only yield the average flow within the cardiac cycle. Nevertheless, the algorithm can also be used to calculate flows for dynamic PC images which need the same components, i.e. generate vessel regions of interest, identify vessels, unalias the vessels, and calculate total CBF. An automated approach to analysis (such as ours) is more important when the number of images increases, such as the case with dynamic PC images. Measures from additional images can be fed back into validation of the algorithm and potentially improve components. The weighting parameters in our algorithm were optimized for our images and can be refined further for other data sets.
We calculated flows only for ICA and VA vessels. Nevertheless, using a gated PC sequence and a lower VENC one could measure blood flow through the deformable internal jugular veins to obtain additional information about CBF on the outflow, thereby evaluating the Monroe-Kelly hypothesis. Alternatively, one could measure flow of other fluids such as cerebrospinal fluid through either the cerebral aqueduct or artificial structures, such as the lumen of a ventriculoperitoneal shunt [29].
We evaluated the performance of 2 image analysts, treating the primary analyst as ground truth when needed. Nevertheless, our objective was an automated alternative that has a similar accuracy to manual analysis yet yields high-precision results. Thus, we can eliminate both inter- and intra-observer variability by replacing human analysts with the algorithm. We did not seek to create yet another demonstration of observer variations in medical image processing, which are well-established.
We did not record the processing time for either the analysts or the algorithm, thus we cannot report the potential time savings of the algorithm. Qualitatively, both analysts noted that generating vessel regions of interest and unaliasing vessels were far more time consuming than identifying vessels and calculating total cerebral blood flow. Both analysts also report that manually processing was fatiguing, requiring them to slow their pace to maintain their quality. These observations suggest that the algorithm might be useful as a clinical support tool for radiologists seeking methods that reduce cognitive burden. Implementing such a tool in clinical practice would require integration with the radiologist workstation software, and consideration for their overall workflow.

Comments (0)