Endovascular flow diversion therapy differs from embolization therapy, which necessitates a specific duration for the formation of new endothelium on the stent surface at the aneurysm neck to achieve occlusion. This approach is not without limitations; not all aneurysms can be occluded or do so within a short timeframe. It is primarily suitable for certain types of aneurysms, underscoring the importance of selecting appropriate candidates based on clinical characteristics to facilitate more rapid and effective aneurysm occlusion.
A retrospective angiographic follow-up analysis of 967 aneurysms from the largest multi-center PED series in China revealed that female, hyperlipidemia, vertebral aneurysms, PED plus coiling, and blood flow detained to venous phase were significant predictors of aneurysm occlusion in multivariate analysis. Conversely, factors such as age, history of SAH, > 6 months dual antiplatelet therapy post-PED implant, aneurysm maximal diameter, and fusiform morphology were associated with incomplete occlusion. For the posterior circulation cohort, there were no variables to compare with [20]. The largest single-center clinical study from Johns Hopkins University School of Medicine conducted a retrospective analysis of 491 cases of PED treatment for anterior circulation aneurysms. Multivariate analysis revealed that at 6 months, advancing age, increasing aneurysm size, history of SAH and adjunctive coiling were significant predictors of aneurysm occlusion; whereas at 12 months, the predictors included male sex, increasing aneurysm size, branch vessel inclusion within the treated aneurysm, along with adjunctive coiling [19]. Another retrospective analysis conducted across 3 experienced vascular centers examined 316 aneurysms treated with PED. Multivariable analysis revealed that older age (> 70 years), greater maximal diameter (≥ 15 mm), and fusiform morphology were strong independently associated with higher rates of incomplete occlusion at last follow-up [18]. In addition to the aforementioned factors, clinical and pathological variables such as location (C4/C5/C6/C7), orientation (concave/convex/flank), H, W, CND, PAD, NR, H/W, AR, BNF, SR, aneurysm volume, ostium area, VOR, and IA have also been incorporated in prior studies to explore their potential association with aneurysm occlusion [17, 20, 26,27,28,29]. It should not be overlooked that the device itself is also an important influencing factor. The respective comparative sizes of the device and the recipient artery, the curvature of the device, as well as the method of deploying the device will affect the porosity of the device, thereby influencing the hemodynamics of the carotid artery carrying the aneurysm, and ultimately affecting aneurysm occlusion, especially in curved vessels such as the carotid siphon [30].
Review of the existing prediction scoring models(FDSS、ABC、DIANES、4 F-FPS) reveals significant variability in the selected variables among them. The Flow Diversion Stent Score (FDSS) is a straightforward outcomes-based scale to characterize results after FD treatment; it assigns points based on age ≥ 60 years (1 point), aneurysm size ≥ 15 mm (1 point), presence of side branches (1 point), and post-treatment Raymond score (1–3 points). Patients with FDSS ≥ 4 were more likely to have residual aneurysm filling on follow-up angiography [21]. The ABC scoring system consisted of: Age (< 60 years old: 0, 60–69 years: 1, 70–79: 2, and ≥ 80: 3), Branch coming out of the aneurysm dome/neck (yes: 2, no: 0), and Cigarette smoking history (never smoker: 1, current or past smoker: 0). A value ≥ 2 proved to be reliable in predicting the risk of incomplete occlusion [31]. The DIANES score employs logistic regression and ML via CART algorithms for feature selection, ultimately 6 significant variables (diameter, indication, parent artery diameter ratio, neck ratio, side-branch artery, and sex) were identified from a pool of 30 pre-treatment features and incorporated into the ML model, demonstrating robust predictive performance. Nevertheless, the study encompasses a limited number of cases, and the scoring parameters are intricate and challenging to remember [23]. In contrast, The Flow Diversion Predictive Score (4 F-FPS) builds upon previously established grading scales (OKM, Kamran, SMART) [25, 32, 33] for angiographic outcomes and identifies 4 critical factors influencing aneurysm occlusion, denoted by the acronym ‘F’: fusiform shape, flow-jet, filling, and final stasis. The scoring system aggregates the scores of these 4 factors, yielding a total score that ranges from 0 to 5. A score of ≥ 3 correlates with an estimated aneurysm occlusion rate of at least 78% [22].
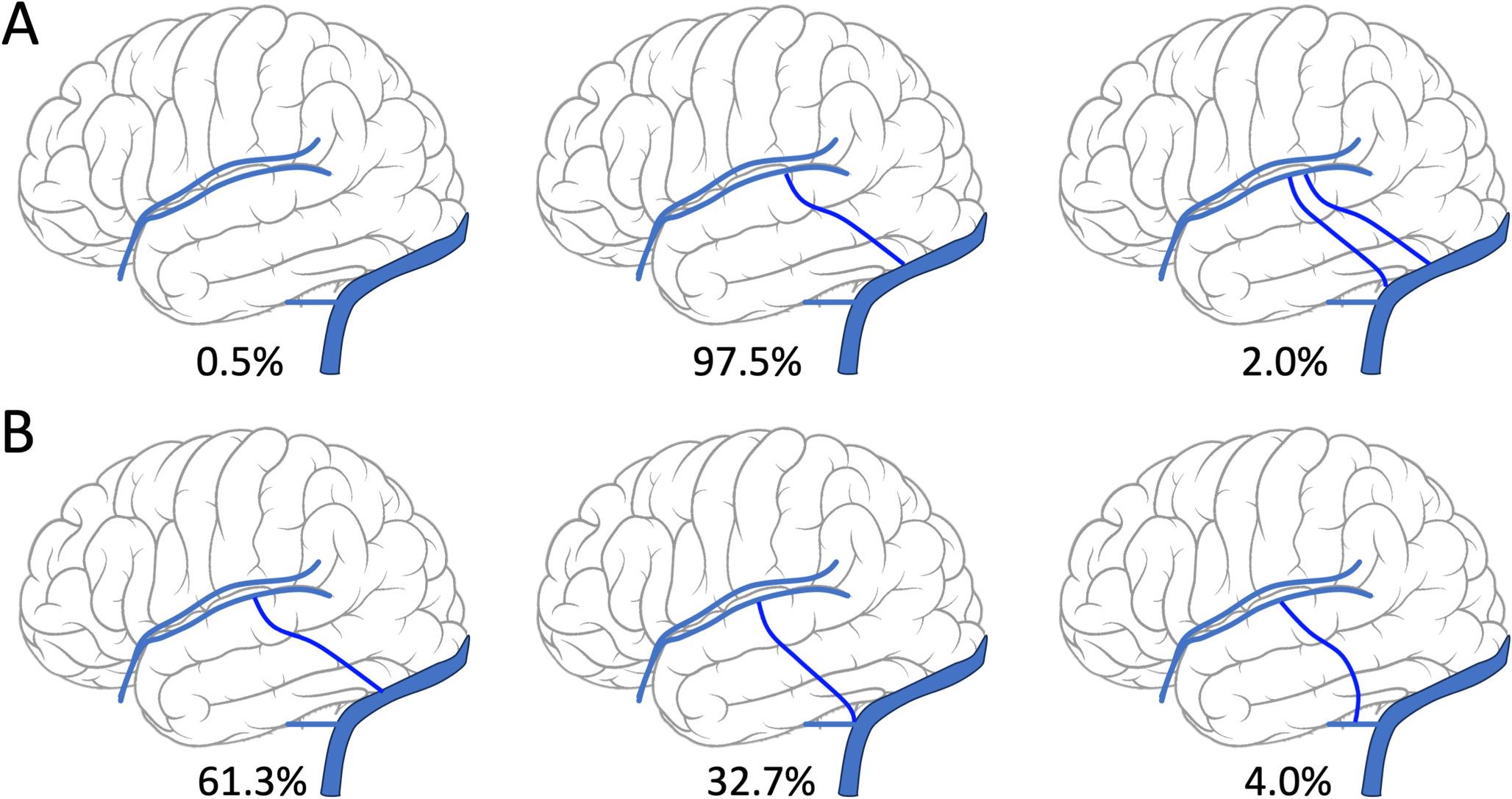
The carotid internal artery siphon segment is not only a high-risk site for aneurysms, but also the main implantation site for blood flow diversion devices. The anatomy of aneurysms at this site is diverse, and the blood flow dynamics are complex [34, 35]. The factors that predict aneurysm closure have not been specifically analyzed. The 4 F-FPS scoring system is excellent, but most of the included factors are angiographic results after FD implantation and can only be used for postoperative prediction. It cannot be used for preoperative assessment of aneurysm occlusion rate, which may not be available for clinical daily practice to provide a reference for the choice of surgical method for a certain aneurysm before operation. ML algorithm shows great predictive power, which distinguishes itself from linear models adopted by previous researches, however, little research in the available literature on applying it to prediction of aneurysm occlusion treated with FD [36, 37]. Based on the above, we conducted further discussions, which is what makes this study different and unique.
This single-center study reviewed data from 342 internal carotid artery siphon aneurysms and conducted univariate and multivariate analyses of the pre-operative characteristic variables, which showed that aneurysm orientation, W, BNF, IA, incorporated branch vessels and adjunct coil deployment were independent influence factors. Meanwhile employing random forest for feature selection analysis facilitates the identification of potentially significant factors. By integrating these findings with previously reported literature, we determined the final variables to be incorporated into the ML model: IA, BNF, incorporated branch vessels, adjunct coil deployment, ostium area, CND, NR, and Dmax.
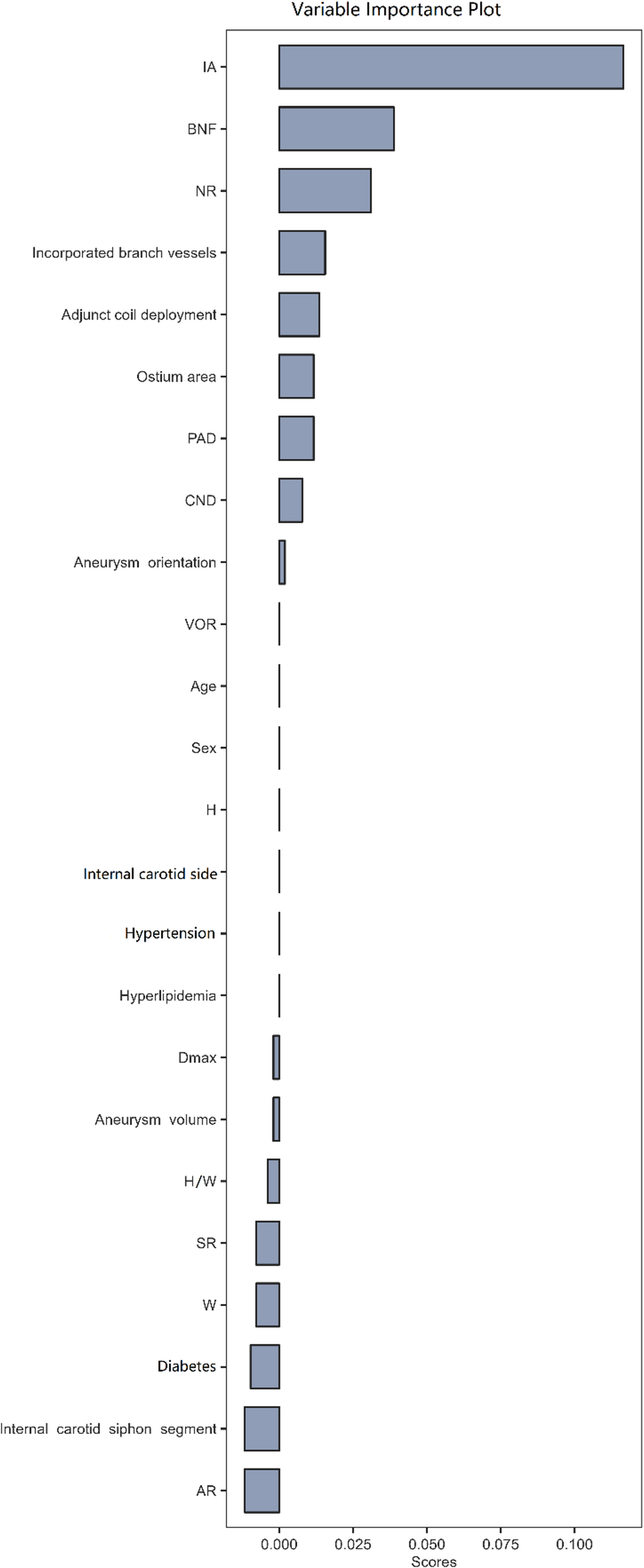
In the ML model applied to the derivation set, the XGBoost algorithm achieved a superior AUROC value of 0.872, followed by GBM at 0.824 and DT at 0.754. This suggests that both XGBoost and GBM algorithms exhibit strong performance on the validation set. Conversely, in the validation set evaluation, The AUROC of GBM is the highest, which can comprehensively evaluate the discrimination ability of the classification model, and several other indicators such as Accuracy and Precision are also superior. This can preliminarily indicate that this model has advantages. The relative importance of variables offers a clear representation of their significance in predicting aneurysm occlusion across various ML algorithms. In descending order of importance within the GBM model, high-ranking variables are as follows: IA, NR, Dmax, adjunct coil deployment, BNF, incorporated branch vessels, CND, and ostium area; where IA, adjunct coil deployment, and BNF serve as positive predictors for aneurysm occlusion while the remaining variables act as negative predictors. These findings appear to align more closely with clinical practice and previous reports. Of course, given the differences in the variables included in the studies by Hammoud [36], as well as in the variable selection for ML and the model training process, the most important predictors also vary. Compared with traditional prediction methods, ML can reduce the dimensionality of a large number of variables, efficiently select the predictive factors with high contribution, and improve the prediction accuracy.
It is noteworthy that there are discernible trends in the evidence: the factor of IA consistently ranks at the top, although significant differences exist regarding the importance of variables among various ML algorithms. IA is recognized as a crucial discriminant for rupture status in sidewall-type aneurysms, computational fluid dynamic analysis showed that increasing IA leading to deeper migration of the flow recirculation zone into the aneurysm with higher peak flow velocities and a greater transmission of kinetic energy into the distal portion of the dome.[38] The association between IA and aneurysm occlusion treated with FD was first reported here; these findings advocate for incorporating IA into future studies. Should these predictive factors be validated across multi-center datasets, it may become feasible to develop specific predictive models and integrate them into user-friendly applications to help predict treatment outcomes in real time. This tool can assist interventionalists in choosing the most appropriate therapeutic modality tailored for each patient, based on clinical risk factors and the morphological characteristics of the aneurysm.
Nevertheless, this study is not without its limitations. Firstly, the nature of a retrospective study might have resulted in selection bias. Secondly, the ML algorithm model we developed was confined to one single institution, which might limit its generality, pending external validation. Lastly, due to the relatively small sample size and model consistency constraints, we did not pursue further development of a predictive scoring system.

Comments (0)